National Centre for Sport and Exercise Medicine, School of Sport, Exercise and Health Sciences, Loughborough University, Loughborough, LE11 3TU, UK.
Office of Student Affairs, Lingnan University, Hong Kong 999077, China; Department of Orthopaedics and Traumatology, Prince of Wales Hospital, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong 999077, China.
J Sport Health Sci. 2023 Jan;12(1):139-144. doi: 10.1016/j.jshs.2021.03.007. Epub 2021 Mar 17.
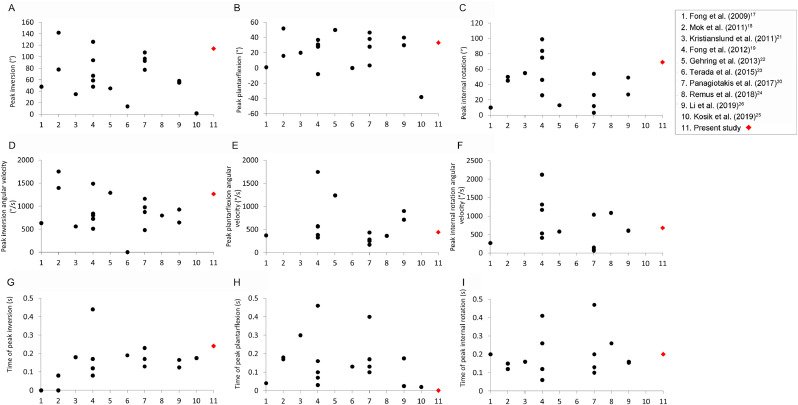
This study presents a kinematic analysis of an acute lateral ankle sprain incurred during a televised badminton match. The kinematics of this injury were compared to those of 19 previously reported cases in the published literature.
Four camera views of an acute lateral ankle sprain incurred during a televised badminton match were synchronized and rendered in 3-dimensional animation software. A badminton court with known dimensions was built in a virtual environment, and a skeletal model scaled to the injured athlete's height was used for skeletal matching. The ankle joint angle and angular velocity profiles of this acute injury were compared to the summarized findings from 19 previously reported cases in the published literature.
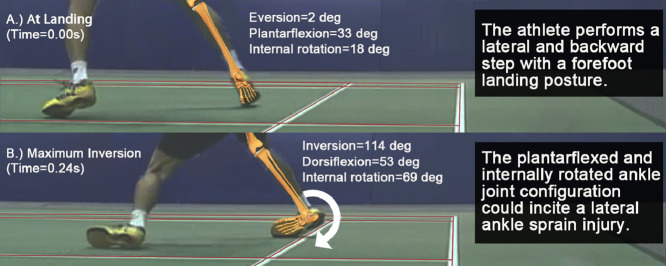
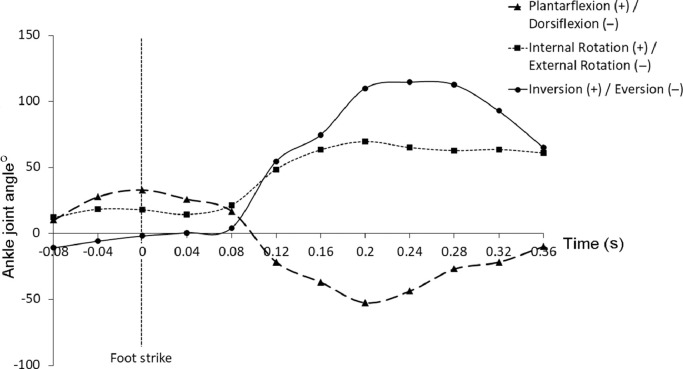
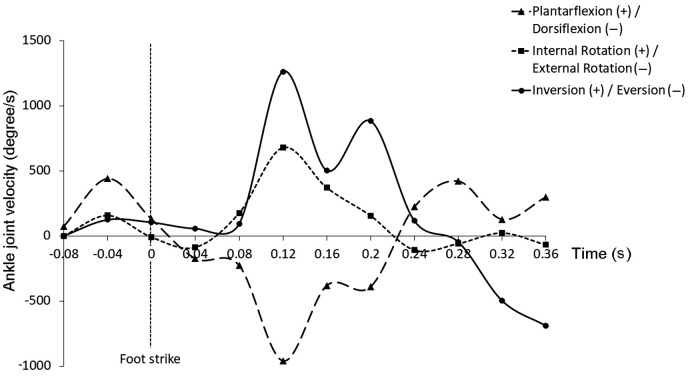
At foot strike, the ankle joint was 2° everted, 33° plantarflexed, and 18° internally rotated. Maximum inversion of 114° and internal rotation of 69° was achieved at 0.24 s and 0.20 s after foot strike, respectively. After the foot strike, the ankle joint moved from an initial position of plantarflexion to dorsiflexion-from 33° plantarflexion to 53° dorsiflexion (range = 86°). Maximum inversion, dorsiflexion, and internal rotation angular velocity were 1262°/s, 961°/s, and 677°/s, respectively, at 0.12 s after foot strike.
A forefoot landing posture with a plantarflexed and internally rotated ankle joint configuration could incite an acute lateral ankle sprain injury in badminton. Prevention of lateral ankle sprains in badminton should focus on the control and stability of the ankle joint angle during forefoot landings, especially when the athletes perform a combined lateral and backward step.
本研究对一起电视转播羽毛球比赛中发生的急性外踝扭伤进行了运动学分析。将该损伤的运动学与已发表文献中 19 例既往报道的病例进行了比较。
对电视转播羽毛球比赛中发生的急性外踝扭伤的四个摄像视角进行了同步处理,并在 3 维动画软件中进行了渲染。在虚拟环境中构建了一个具有已知尺寸的羽毛球场地,并使用与受伤运动员身高成比例的骨骼模型进行骨骼匹配。将该急性损伤的踝关节角度和角速度曲线与已发表文献中 19 例既往报道病例的汇总发现进行了比较。
在足着地时,踝关节外旋 2°,跖屈 33°,内旋 18°。最大内翻 114°和内旋 69°分别在足着地后 0.24 s 和 0.20 s 时达到。足着地后,踝关节从初始跖屈位置移动到背屈位置——从 33°跖屈到 53°背屈(范围为 86°)。最大内翻、背屈和内旋角速度分别为 0.12 s 时的 1262°/s、961°/s 和 677°/s。
前足着地时,踝关节跖屈和内旋的姿势可能会导致羽毛球运动中发生急性外踝扭伤。预防羽毛球中外侧踝关节扭伤应重点控制和稳定前足着地时的踝关节角度,特别是运动员进行侧向和向后跨步时。