UPMC Hillman Cancer Center, Pittsburgh, Pennsylvania.
University of Pittsburgh, Pittsburgh, Pennsylvania.
Clin Cancer Res. 2021 Aug 1;27(15):4195-4204. doi: 10.1158/1078-0432.CCR-20-4301. Epub 2021 Mar 22.
Neoadjuvant immunotherapy may improve the clinical outcome of regionally advanced operable melanoma and allows for rapid clinical and pathologic assessment of response. We examined neoadjuvant pembrolizumab and high-dose IFNα-2b (HDI) therapy in patients with resectable advanced melanoma.
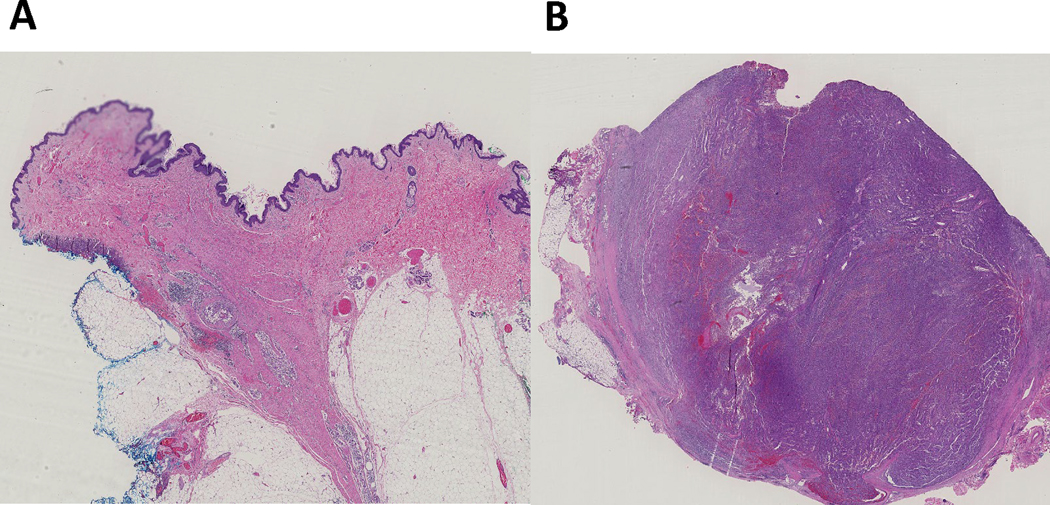
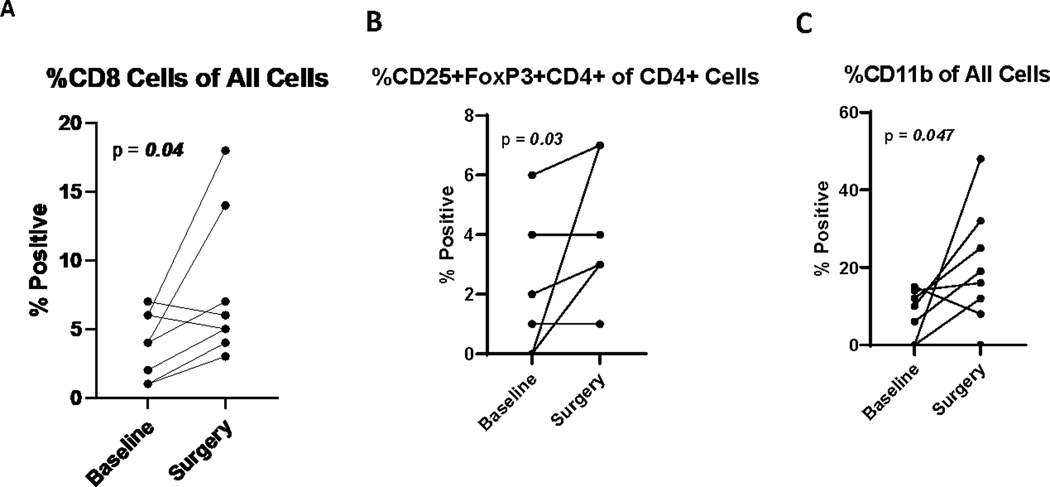
Patients with resectable stage III/IV melanoma were treated with concurrent pembrolizumab 200 mg i.v. every 3 weeks and HDI 20 MU/m/day i.v., 5 days per week for 4 weeks, then 10 MU/m/day subcutaneously 3 days per week for 2 weeks. Definitive surgery followed, as did adjuvant combination immunotherapy, completing a year of treatment. Primary endpoint was safety of the combination. Secondary endpoints included overall response rate (ORR), pathologic complete response (pCR), recurrence-free survival (RFS), and overall survival (OS). Blood samples for correlative studies were collected throughout. Tumor tissue was assessed by IHC and flow cytometry at baseline and at surgery.
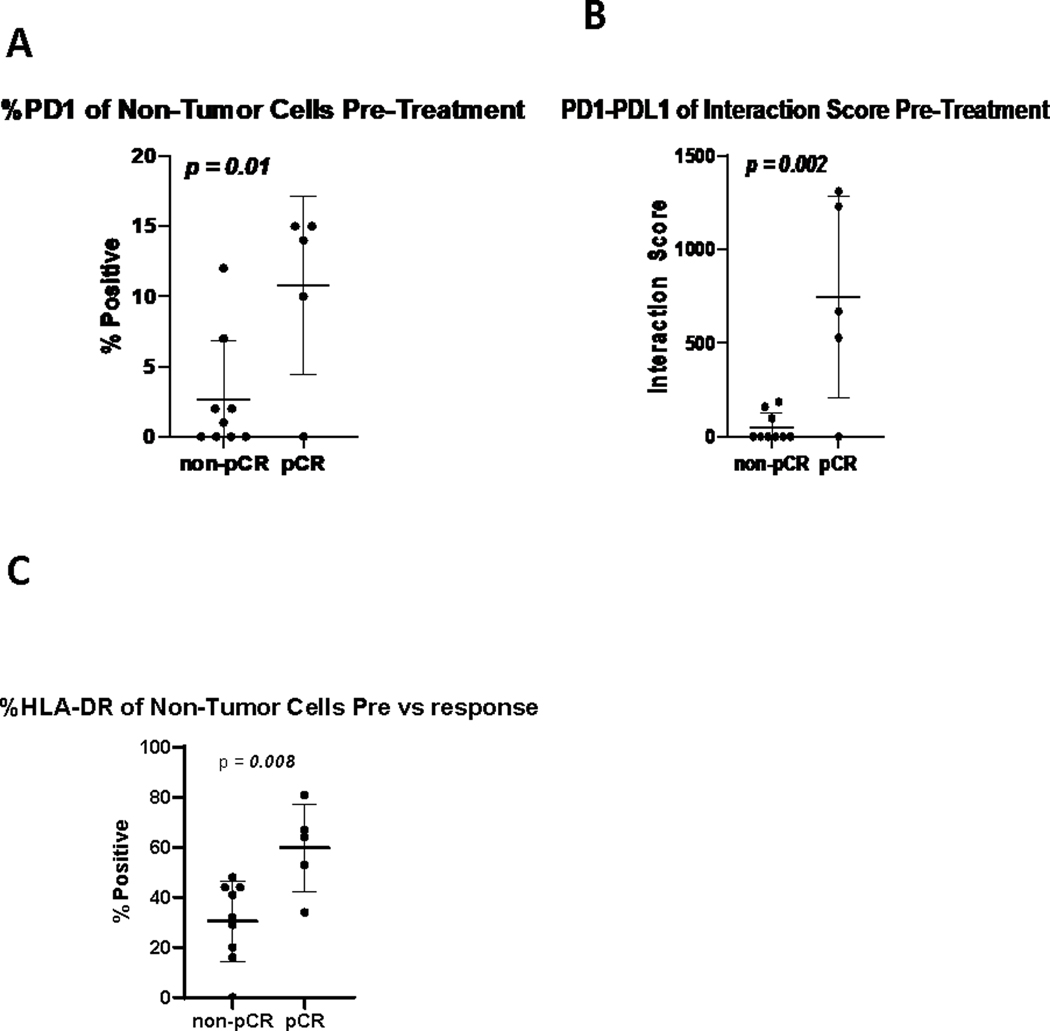
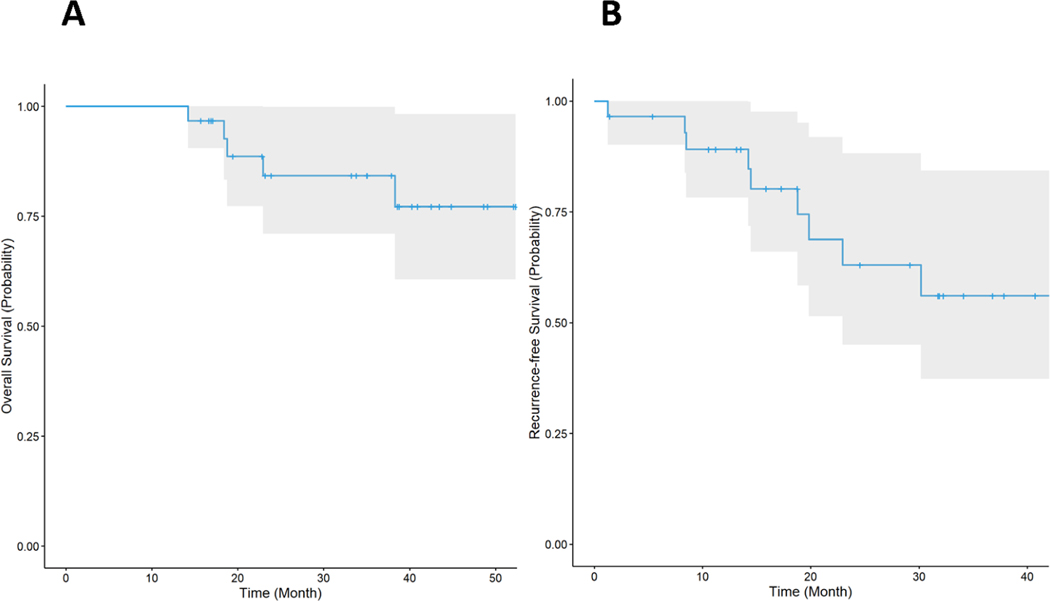
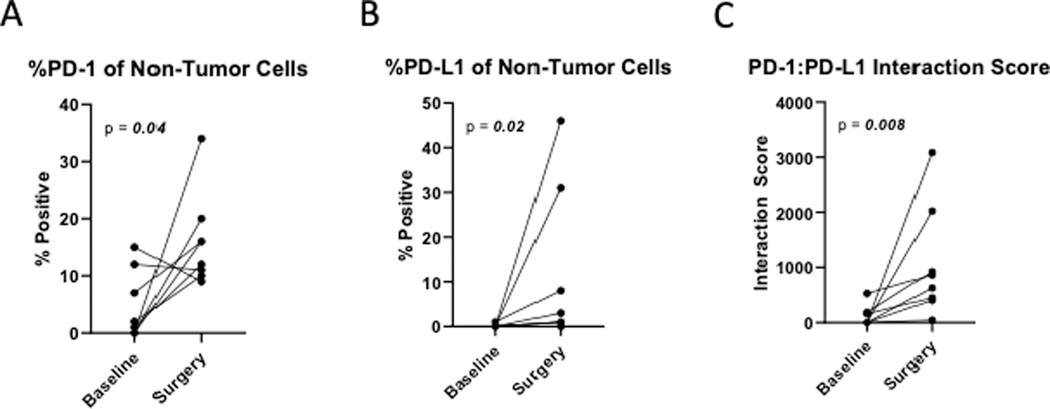
A total of 31 patients were enrolled, and 30 were evaluable. At data cutoff (October 2, 2019), median follow-up for OS was 37.87 months (range, 33.2-43.47). Median OS and RFS were not reached. Radiographic ORR was 73.3% [95% confidence interval (CI): 55.5-85.8], with a 43% (95% CI: 27.3-60.1) pCR rate. None of the patients with a pCR have had a recurrence. HDI and pembrolizumab were discontinued in 73% and 43% of patients, respectively. Correlative analyses suggested that intratumoral PD-1/PD-L1 interaction and HLA-DR expression are associated with pCR ( = 0.002 and = 0.008, respectively).
Neoadjuvant concurrent HDI and pembrolizumab demonstrated promising clinical activity despite high rates of treatment discontinuation. pCR is a prognostic indicator..
新辅助免疫疗法可能改善局部晚期可手术黑色素瘤的临床结局,并能快速进行临床和病理反应评估。我们研究了可切除的晚期黑色素瘤患者新辅助派姆单抗和高剂量 IFNα-2b(HDI)治疗。
可切除的 III/IV 期黑色素瘤患者接受新辅助派姆单抗 200mg 静脉注射,每 3 周一次,同时给予 HDI 20MU/m/天静脉注射,每周 5 天,共 4 周,然后皮下给予 10MU/m/天,每周 3 天,共 2 周。随后进行确定性手术,并进行辅助联合免疫治疗,共治疗 1 年。主要终点是联合治疗的安全性。次要终点包括总缓解率(ORR)、病理完全缓解(pCR)、无复发生存率(RFS)和总生存率(OS)。在整个研究过程中收集了用于相关性研究的血液样本。基线时和手术时通过免疫组化和流式细胞术评估肿瘤组织。
共纳入 31 例患者,30 例可评估。截至数据截止日期(2019 年 10 月 2 日),OS 的中位随访时间为 37.87 个月(范围 33.2-43.47)。中位 OS 和 RFS 尚未达到。影像学 ORR 为 73.3%(95%可信区间:55.5-85.8),pCR 率为 43%(95%可信区间:27.3-60.1)。没有 pCR 的患者均未复发。分别有 73%和 43%的患者停用了 HDI 和派姆单抗。相关性分析表明,肿瘤内 PD-1/PD-L1 相互作用和 HLA-DR 表达与 pCR 相关(分别为 = 0.002 和 = 0.008)。
尽管治疗中断率较高,但新辅助同时给予 HDI 和派姆单抗显示出有希望的临床活性。pCR 是预后指标。