Department of Cardiology, Heart Center, University of Cologne, Kerpener Str. 62, 50937, Cologne, Germany.
Department of Cardiothoracic Surgery, Heart Center, University of Cologne, Kerpener Str. 62, 50937, Cologne, Germany.
Clin Res Cardiol. 2022 May;111(5):492-501. doi: 10.1007/s00392-021-01826-x. Epub 2021 Mar 23.
In patients with severe aortic stenosis (AS) undergoing transcatheter aortic valve implantation (TAVI) and heart failure with severely reduced ejection fraction, prediction of postprocedural left ventricular ejection fraction (LVEF) improvement is challenging. Decision-making and timing for implantable cardioverter defibrillator (ICD) treatment are difficult and benefit is still unclear in this patient population.
Aims of the study were to analyse long-term overall mortality in TAVI-patients with a preprocedural LVEF ≤ 35% regarding LVEF improvement and effect of ICD therapy.
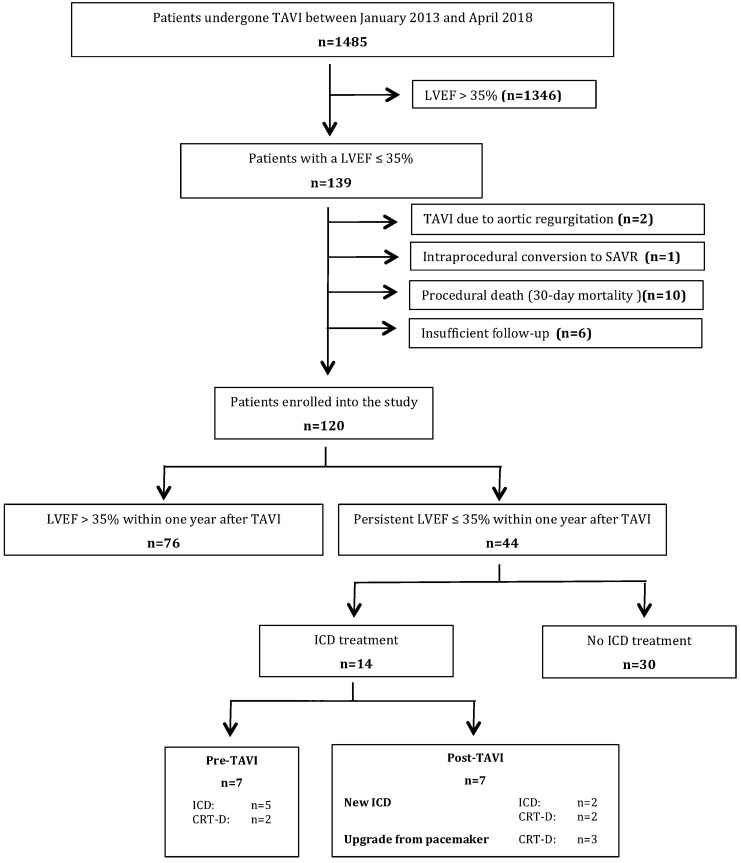
Retrospective analysis of a high-risk TAVI-population suffering from severe AS and heart failure with a LVEF ≤ 35%. Out of 1485 TAVI-patients treated at this center between January 2013 and April 2018, 120 patients revealed a preprocedural LVEF ≤ 35% and had sufficient follow-up. 36.7% (44/120) of the patients suffered from persistent reduced LVEF without a postprocedural increase above 35% within 1 year after TAVI or before death, respectively. Overall mortality was neither significantly reduced by LVEF recovery above 35% (p = 0.31) nor by additional ICD treatment in patients with persistent LVEF ≤ 35% (p = 0.33).
In high-risk TAVI-patients suffering from heart failure with LVEF ≤ 35%, LVEF improvement to more than 35% did not reduce overall mortality. Patients with postprocedural persistent LVEF reduction did not seem to benefit from ICD treatment. Effects of LVEF improvement and ICD treatment on mortality are masked by the competing risk of death from relevant comorbidities.
在接受经导管主动脉瓣置换术(TAVI)和射血分数严重降低的心力衰竭的严重主动脉瓣狭窄(AS)患者中,预测术后左心室射血分数(LVEF)的改善具有挑战性。在该患者人群中,决定是否植入植入式心脏复律除颤器(ICD)以及其获益仍不明确。
本研究旨在分析术前 LVEF≤35%的 TAVI 患者的 LVEF 改善情况和 ICD 治疗的长期总死亡率。
对在该中心于 2013 年 1 月至 2018 年 4 月期间接受治疗的高危 TAVI 人群进行回顾性分析,这些患者患有严重的 AS 和射血分数≤35%的心力衰竭。在该中心接受治疗的 1485 例 TAVI 患者中,有 120 例患者的术前 LVEF≤35%且随访资料完整。在这 120 例患者中,有 36.7%(44/120)的患者在 TAVI 后 1 年内或死亡前的持续 LVEF 没有增加,且 LVEF 未恢复至 35%以上。LVEF 恢复至 35%以上(p=0.31)或持续 LVEF≤35%的患者接受 ICD 治疗(p=0.33)均不能显著降低总死亡率。
在患有射血分数≤35%的心力衰竭的高危 TAVI 患者中,LVEF 改善至 35%以上并不能降低总死亡率。术后持续 LVEF 降低的患者似乎不能从 ICD 治疗中获益。LVEF 改善和 ICD 治疗对死亡率的影响被相关合并症导致的死亡竞争风险所掩盖。