Second Department of Internal Medicine.
Clinical Study Support Center, Wakayama Medical University, Wakayama.
Medicine (Baltimore). 2021 Mar 26;100(12):e25268. doi: 10.1097/MD.0000000000025268.
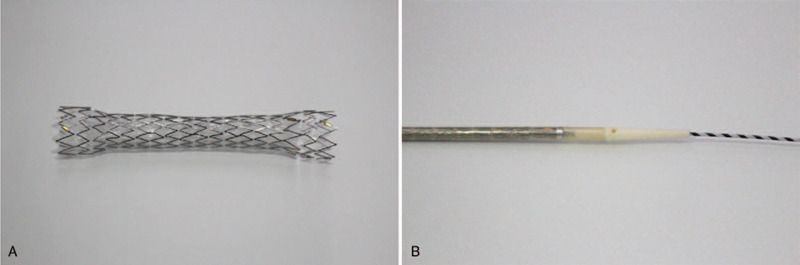
In patients with malignant distal bile duct obstruction and normal gastrointestinal anatomy, endoscopic ultrasound-guided choledochoduodenostomy (EUS-CDS) is indicated when endoscopic retrograde cholangiopancreatography (ERCP) fails. The ERCP drainage route passes through the tumor, whereas the EUS-CDS route does not. Therefore, EUS-CDS is expected to have a longer stent patency than ERCP. However, for first-line biliary drainage, it remains unclear whether EUS-CDS or ERCP is superior in terms of stent patency. To reduce the frequency of highly adverse events (AEs) such as bile peritonitis or stent migration following EUS-CDS, we developed an antimigration metal stent with a thin delivery system for tract dilatation. This study is designed to assess whether EUS-CDS with this novel stent is superior to ERCP with a traditional metal stent in terms of stent patency when the two techniques are used for first-line drainage of malignant distal biliary obstruction.
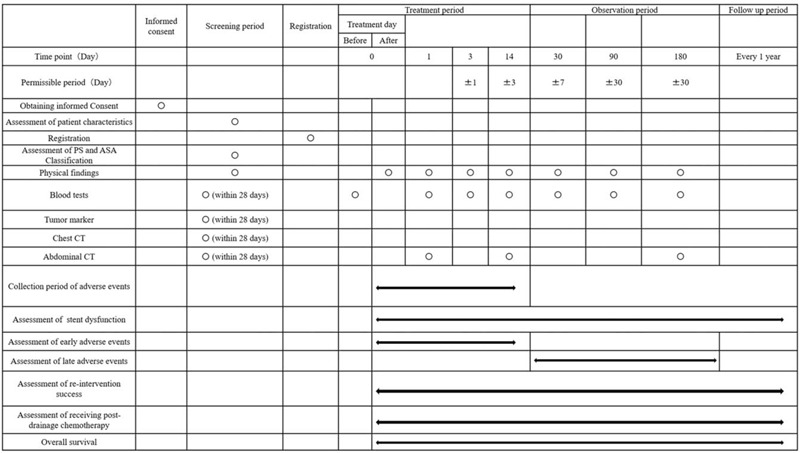
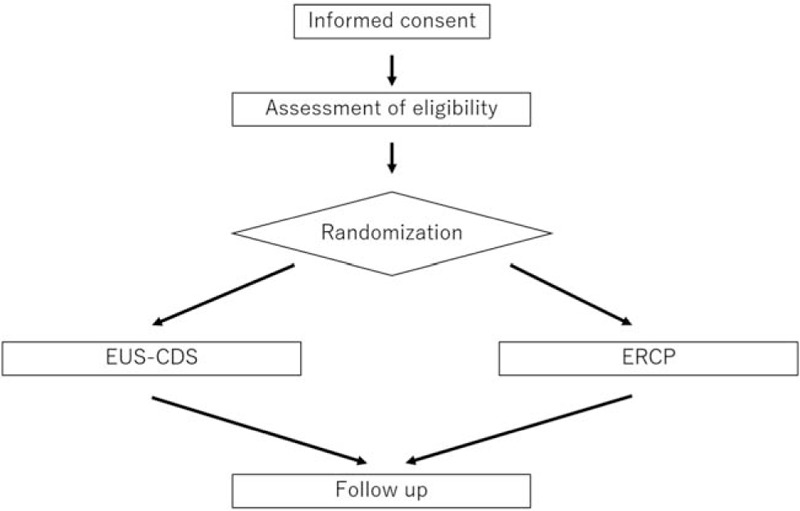
METHODS/DESIGN: This study is a multicenter single-blinded randomized controlled trial (RCT) involving 95 patients in four tertiary centers. Patients with malignant distal biliary obstruction that is unresectable or presents a very high surgical risk and who pass the inclusion and exclusion criteria will be randomized to EUS-CDS or ERCP in a 1:1 proportion. The primary endpoint is the stent patency rate 180 days after stent insertion. Secondary outcomes include the rates of technical success, clinical success, technical success in cases not requiring fistulous-tract dilation (only EUS-CDS group), procedure-related AEs, re-intervention success, patients receiving post-drainage chemotherapy, procedure time, and overall survival time.
If EUS-CDS is superior to ERCP in terms of stent patency and safety for the first-line drainage of malignant distal biliary obstruction, it is expected that the first-line drainage method will be changed from ERCP to EUS-CDS, and that interruption of chemotherapy due to stent dysfunction can be avoided.
University Hospital Medical Information Network Clinical Trials Registry (UMIN-CTR), ID: UMIN000041343. Registered on August 6, 2020. https://upload.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000047201Version number: 1.2, December 7, 2020.
在患有恶性远端胆管梗阻且胃肠道解剖结构正常的患者中,如果内镜逆行胰胆管造影术 (ERCP) 失败,则应进行内镜超声引导下胆肠吻合术 (EUS-CDS)。ERCP 的引流途径穿过肿瘤,而 EUS-CDS 的途径则不穿过肿瘤。因此,EUS-CDS 预计支架通畅时间会比 ERCP 更长。然而,对于一线胆道引流,目前尚不清楚 EUS-CDS 与 ERCP 哪一种在支架通畅方面更具优势。为了降低 EUS-CDS 后胆汁性腹膜炎或支架迁移等高度不良事件 (AE) 的发生频率,我们开发了一种带有薄输送系统的防迁移金属支架,用于扩张通道。本研究旨在评估当两种技术用于恶性远端胆管梗阻的一线引流时,使用这种新型支架的 EUS-CDS 是否优于 ERCP 联合传统金属支架,在支架通畅方面更具优势。
方法/设计:这是一项涉及四家三级中心的 95 名患者的多中心单盲随机对照试验 (RCT)。将符合纳入和排除标准且不可切除或手术风险极高的恶性远端胆管梗阻患者随机分为 EUS-CDS 组或 ERCP 组,比例为 1:1。主要终点是支架植入后 180 天的支架通畅率。次要结局包括技术成功率、临床成功率、无需瘘道扩张的技术成功率(仅 EUS-CDS 组)、与操作相关的 AE 发生率、再介入成功率、接受引流后化疗的患者比例、操作时间和总生存时间。
如果 EUS-CDS 在恶性远端胆管梗阻的一线引流中在支架通畅性和安全性方面优于 ERCP,则预计一线引流方法将从 ERCP 改为 EUS-CDS,并且可以避免因支架功能障碍而中断化疗。
大学医院医疗信息网络临床试验注册(UMIN-CTR),ID:UMIN000041343。注册于 2020 年 8 月 6 日。https://upload.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000047201。版本号:1.2,2020 年 12 月 7 日。