Department of Cardiology and Cardiovascular Research Institute Basel (CRIB), University Hospital Basel, University of Basel, Spitalstrasse 2, CH-4056, Basel, Switzerland.
Interdisciplinary Medicine in Cardiology Unit, Cardiology Department, Heart Institute (InCor), University of Sao Paulo Medical School, São Paulo, Brazil.
Clin Res Cardiol. 2021 Sep;110(9):1450-1463. doi: 10.1007/s00392-021-01827-w. Epub 2021 Mar 25.
Perioperative myocardial infarction/injury (PMI) diagnosed by high-sensitivity troponin (hs-cTn) T is frequent and a prognostically important complication of non-cardiac surgery. We aimed to evaluate the incidence and outcome of PMI diagnosed using hs-cTnI, and compare it to PMI diagnosed using hs-cTnT.
We prospectively included 2455 patients at high cardiovascular risk undergoing 3111 non-cardiac surgeries, for whom hs-cTnI and hs-cTnT concentrations were measured before surgery and on postoperative days 1 and 2. PMI was defined as a composite of perioperative myocardial infarction (PMI) and perioperative myocardial injury (PMI), according to the Fourth Universal Definition of Myocardial Infarction. All-cause mortality was the primary endpoint.
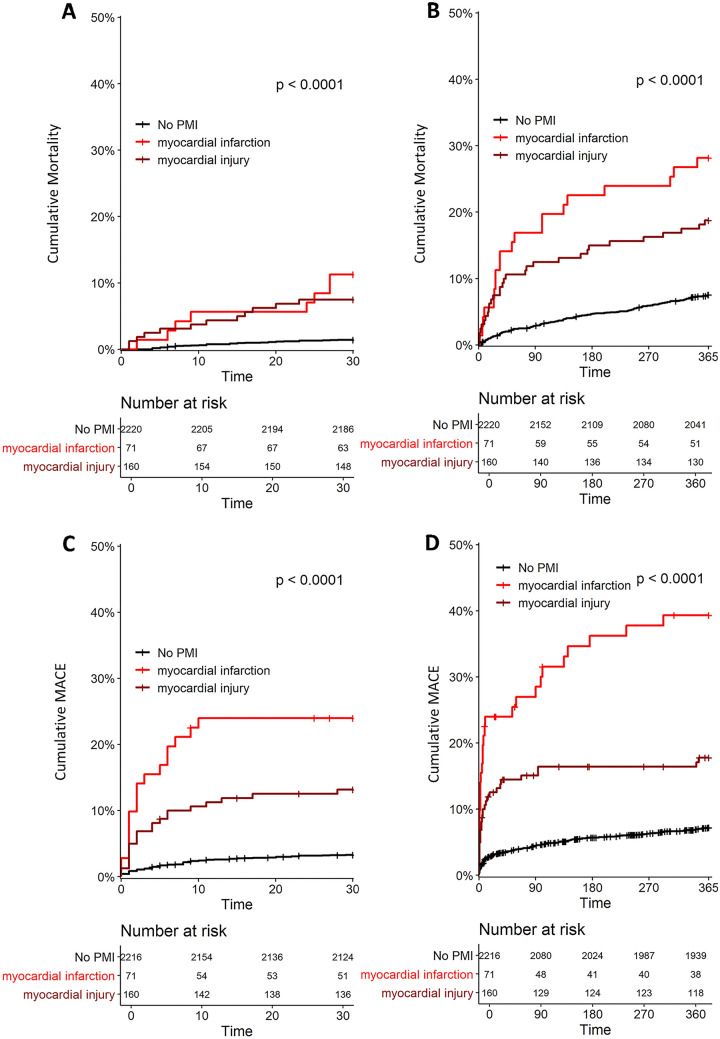
Using hs-cTnI, the incidence of overall PMI was 9% (95% confidence interval [CI] 8-10%), including PMI 2.6% (95% CI 2.0-3.2) and PMI 6.1% (95% CI 5.3-6.9%), which was lower versus using hs-cTnT: overall PMI 15% (95% CI 14-16%), PMI 3.7% (95% CI 3.0-4.4) and PMI 11.3% (95% CI 10.2-12.4%). All-cause mortality occurred in 52 (2%) patients within 30 days and 217 (9%) within 1 year. Using hs-cTnI, both PMI and PMI were independent predictors of 30-day all-cause mortality (adjusted hazard ratio [aHR] 2.5 [95% CI 1.1-6.0], and aHR 2.8 [95% CI 1.4-5.5], respectively) and, 1-year all-cause mortality (aHR 2.0 [95% CI 1.2-3.3], and aHR 1.8 [95% CI 1.2-2.7], respectively). Overall, the prognostic impact of PMI diagnosed by hs-cTnI was comparable to the prognostic impact of PMI using hs-cTnT.
Using hs-cTnI, PMI is less common versus using hs-cTnT. Using hs-cTnI, both PMI and PMI remain independent predictors of 30-day and 1-year mortality.
通过高敏肌钙蛋白(hs-cTn)T 诊断的围手术期心肌梗死/损伤(PMI)是非心脏手术的一种常见且具有重要预后意义的并发症。我们旨在评估使用 hs-cTnI 诊断的 PMI 的发生率和结局,并与使用 hs-cTnT 诊断的 PMI 进行比较。
我们前瞻性纳入了 2455 例心血管高危患者,他们接受了 3111 例非心脏手术,在术前和术后第 1 天及第 2 天检测 hs-cTnI 和 hs-cTnT 浓度。根据第四版心肌梗死通用定义,将围手术期心肌梗死(PMI)和围手术期心肌损伤(PMI)的复合定义为 PMI。全因死亡率为主要终点。
使用 hs-cTnI,总体 PMI 的发生率为 9%(95%CI 8-10%),包括 PMI 2.6%(95%CI 2.0-3.2)和 PMI 6.1%(95%CI 5.3-6.9%),低于使用 hs-cTnT:总体 PMI 为 15%(95%CI 14-16%)、PMI 为 3.7%(95%CI 3.0-4.4%)和 PMI 为 11.3%(95%CI 10.2-12.4%)。术后 30 天内有 52 例(2%)患者和术后 1 年内有 217 例(9%)患者发生全因死亡。使用 hs-cTnI,PMI 和 PMI 均为术后 30 天全因死亡率的独立预测因素(校正后危险比[aHR] 2.5[95%CI 1.1-6.0]和 aHR 2.8[95%CI 1.4-5.5])和术后 1 年全因死亡率的独立预测因素(aHR 2.0[95%CI 1.2-3.3]和 aHR 1.8[95%CI 1.2-2.7])。总体而言,使用 hs-cTnI 诊断的 PMI 的预后影响与使用 hs-cTnT 诊断的 PMI 的预后影响相当。
与使用 hs-cTnT 相比,使用 hs-cTnI 时 PMI 发生率较低。使用 hs-cTnI,PMI 和 PMI 均为术后 30 天和 1 年死亡率的独立预测因素。