Hall Bradley R, Egr Zachary H, Krell Robert W, Padussis James C, Shostrom Valerie K, Are Chandrakanth, Reames Bradley N
Division of Surgical Oncology, Department of Surgery, University of Nebraska Medical Center, 986880 Nebraska Medical Center, Omaha, NE, 68198, USA.
College of Medicine, University of Nebraska, Omaha, NE, USA.
World J Surg Oncol. 2021 Apr 14;19(1):118. doi: 10.1186/s12957-021-02227-0.
The optimal type of operative drainage following pancreaticoduodenectomy (PD) remains unclear. Our objective is to investigate risk associated with closed drainage techniques (passive [gravity] vs. suction) after PD.
We assessed operative drainage techniques utilized in patients undergoing PD in the ACS-NSQIP pancreas-targeted database from 2016 to 2018. Using multivariable logistic regression to adjust for characteristics of the patient, procedure, and pancreas, we examined the association between use of gravity drainage and postoperative outcomes.
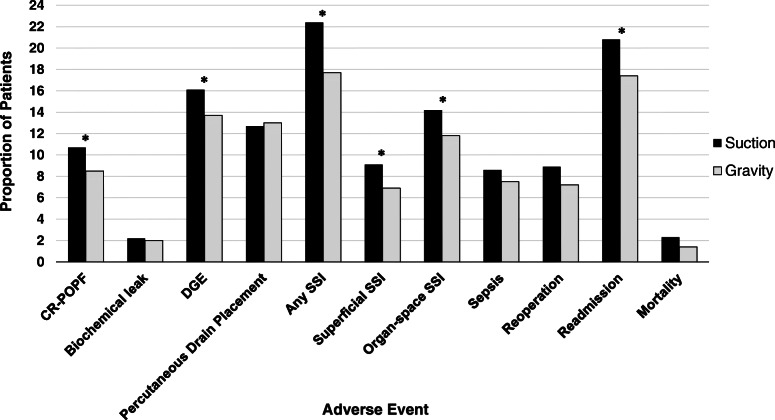
We identified 9665 patients with drains following PD from 2016 to 2018, of which 12.7% received gravity drainage. 61.0% had a diagnosis of adenocarcinoma or pancreatitis, 26.5% had a duct <3 mm, and 43.5% had a soft or intermediate gland. After multivariable adjustment, gravity drainage was associated with decreased rates of postoperative pancreatic fistula (odds ratio [OR] 0.779, 95% confidence interval [CI] 0.653-0.930, p=0.006), delayed gastric emptying (OR 0.830, 95% CI 0.693-0.988, p=0.036), superficial SSI (OR 0.741, 95% CI 0.572-0.959, p=0.023), organ space SSI (OR 0.791, 95% CI 0.658-0.951, p=0.012), and readmission (OR 0.807, 95% CI 0.679-0.958, p=0.014) following PD.
Gravity drainage is independently associated with decreased rates of CR-POPF, DGE, SSI, and readmission following PD. Additional prospective research is necessary to better understand the preferred drainage technique following PD.
胰十二指肠切除术(PD)后最佳的手术引流方式仍不明确。我们的目的是研究PD后闭式引流技术(被动[重力]引流与负压吸引)相关的风险。
我们评估了2016年至2018年美国外科医师学会国家外科质量改进计划(ACS-NSQIP)胰腺靶向数据库中接受PD患者所采用的手术引流技术。使用多变量逻辑回归来调整患者、手术和胰腺的特征,我们研究了重力引流的使用与术后结局之间的关联。
我们在2016年至2018年期间识别出9665例PD后留置引流管的患者,其中12.7%接受重力引流。61.0%的患者诊断为腺癌或胰腺炎,26.5%的患者胰管<3mm,43.5%的患者胰腺质地柔软或中等。多变量调整后,重力引流与PD后术后胰瘘发生率降低相关(比值比[OR]0.779,95%置信区间[CI]0.653 - 0.930,p = 0.006)、胃排空延迟(OR 0.830,95% CI 0.693 - 0.988,p = 0.036)、浅表手术部位感染(SSI)(OR 0.741,95% CI 0.572 - 0.959,p = 0.023)、器官腔隙SSI(OR 0.791,95% CI 0.658 - 0.951,p = 0.012)以及再入院率(OR 0.807,95% CI 0.679 - 0.958,p = 0.014)相关。
重力引流与PD后临床相关胰瘘(CR-POPF)、胃排空延迟(DGE)、手术部位感染(SSI)和再入院率降低独立相关。需要进一步的前瞻性研究以更好地了解PD后的首选引流技术。