Zhao Chen-Guang, Sun Wei, Ju Fen, Jiang Shan, Wang Hong, Sun Xiao-Long, Mou Xiang, Yuan Hua
Department of Rehabilitation Medicine, Xijing Hospital, Fourth Military Medical University, Xi'an, China.
Department of Rehabilitation Medicine, China-Japan Friendship Hospital, Beijing, China.
Pain Ther. 2021 Dec;10(2):1085-1100. doi: 10.1007/s40122-021-00261-0. Epub 2021 Apr 17.
Central poststroke pain (CPSP) develops commonly after stroke, which impairs the quality of life, mood, and social functioning. Current pharmacological approaches for the treatment of CPSP are not satisfactory. Repetitive transcranial magnetic stimulation (rTMS) is a noninvasive technique which has been recommended for the treatment of chronic CPSP. However, few studies have evaluated the analgesic effects of rTMS in patients with acute neuropathic pain after stroke.
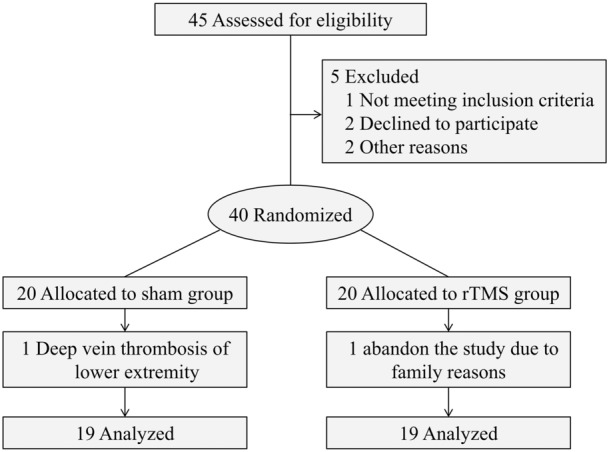
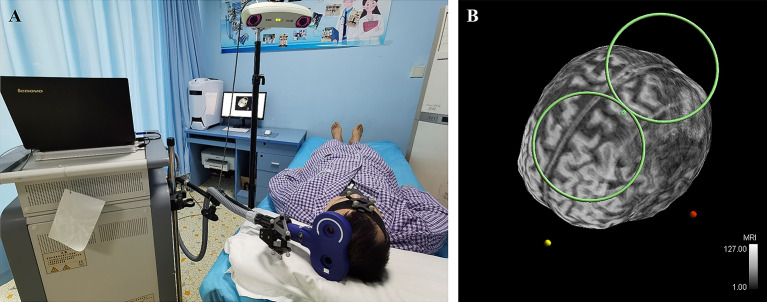
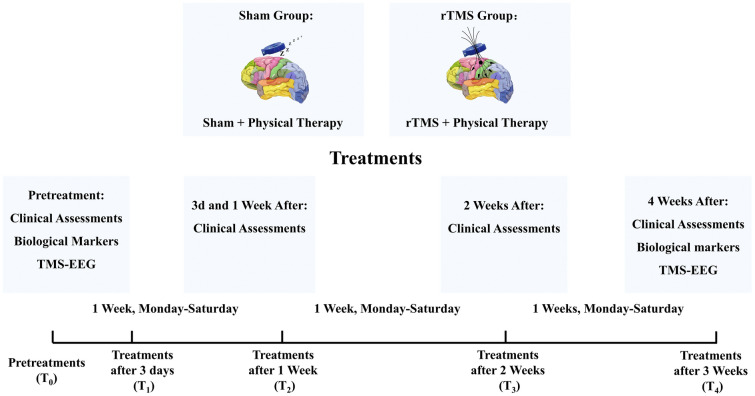
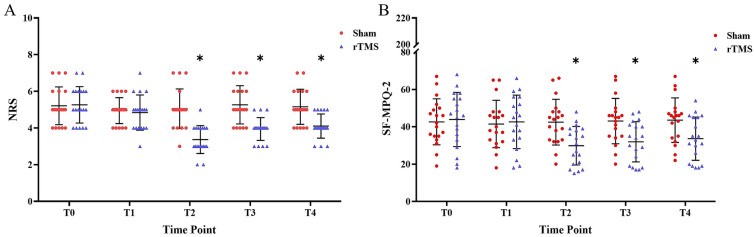
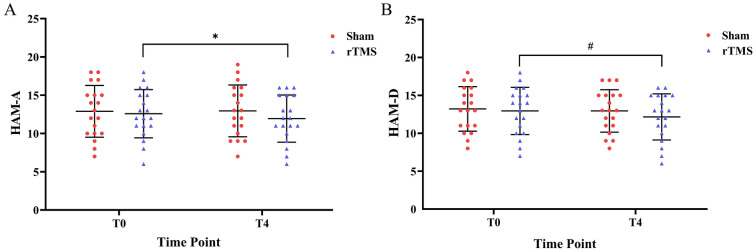
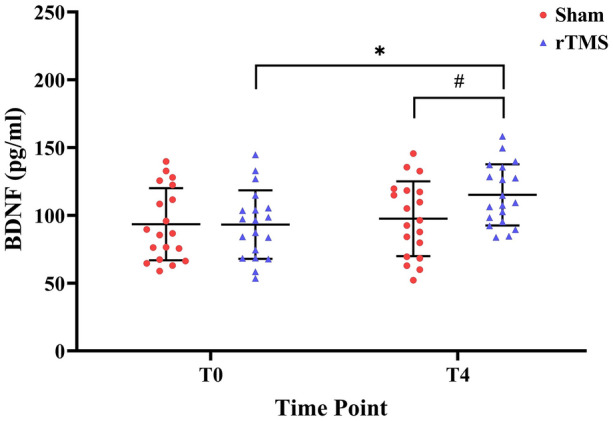
We evaluated the analgesic effects of rTMS applied over the upper extremity area of the motor cortex (M1) in patients with acute CPSP. Forty patients were randomized to receive either rTMS (10 Hz, 2000 stimuli) (n = 20) or a sham intervention (n = 20) for 3 weeks. The Numeric Rating Scale (NRS), Short-form McGill Pain Questionnaire-2 (SF-MPQ-2, Chinese version), Hamilton Anxiety Scale (HAM-A), Hamilton Depression Scale (HAM-D), brain-derived neurotrophic factor (BDNF) levels, and motor-evoked potentials (MEP) were analyzed at baseline, 3 days, 1 week, 2 weeks, and 3 weeks.
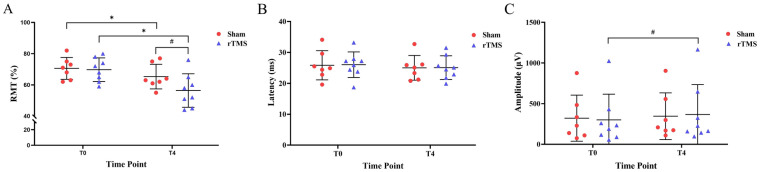
Significant treatment-time interactions were found for pain intensity. Compared with the sham group, the NRS and SF-MPQ-2 scores were significantly lower on the seventh day of treatment in the rTMS group (P < 0.001, Cohen's d = 1.302) (P = 0.003, Cohen's d = 0.771), and this effect lasted until the third week (P = 0.001, Cohen's d = 0.860) (P = 0.027, Cohen's d = 0.550). The HAM-A and HAM-D scores did not change in the rTMS group when compared with the sham group (P = 0.341, Cohen's d = 0.224) (P = 0.356, Cohen's d = 0.217). The serum BDNF levels were significantly higher in the treated group (P = 0.048, Cohen's d = -0.487), and the resting motor threshold (RMT) decreased by 163.65%.
Our findings indicate that rTMS applied over the upper extremity area of the motor cortex can effectively alleviate acute CPSP, possibly by influencing cortical excitability and serum BDNF secretion.
This trial is registered with Clinical Trial Registry of China: Reg. No. ChiCTR-INR-17012880.
中风后中枢性疼痛(CPSP)在中风后很常见,会损害生活质量、情绪和社会功能。目前用于治疗CPSP的药物方法并不令人满意。重复经颅磁刺激(rTMS)是一种非侵入性技术,已被推荐用于治疗慢性CPSP。然而,很少有研究评估rTMS对中风后急性神经性疼痛患者的镇痛效果。
我们评估了在急性CPSP患者的运动皮层(M1)上肢区域应用rTMS的镇痛效果。40例患者被随机分为接受rTMS(10Hz,2000次刺激)(n = 20)或假干预(n = 20),为期3周。在基线、3天、1周、2周和3周时分析数字评分量表(NRS)、简化麦吉尔疼痛问卷-2(SF-MPQ-2,中文版)、汉密尔顿焦虑量表(HAM-A)、汉密尔顿抑郁量表(HAM-D)、脑源性神经营养因子(BDNF)水平和运动诱发电位(MEP)。
在疼痛强度方面发现了显著的治疗时间交互作用。与假手术组相比,rTMS组在治疗第7天时NRS和SF-MPQ-2评分显著更低(P < 0.001,Cohen's d = 1.302)(P = 0.003,Cohen's d = 0.771),且这种效果持续到第3周(P = 0.001,Cohen's d = 0.860)(P = 0.027,Cohen's d = 0.550)。与假手术组相比,rTMS组的HAM-A和HAM-D评分没有变化(P = 0.341,Cohen's d = 0.224)(P = 0.356,Cohen's d = 0.217)。治疗组血清BDNF水平显著更高(P = 0.048,Cohen's d = -0.487),静息运动阈值(RMT)下降了163.65%。
我们的研究结果表明,在运动皮层上肢区域应用rTMS可有效缓解急性CPSP,可能是通过影响皮层兴奋性和血清BDNF分泌。
本试验在中国临床试验注册中心注册:注册号ChiCTR-INR-17012880。