Koch Aleksander, Krasny Joanna, Dziurda Magdalena, Ratajczyk Magdalena, Jozwiak Marek
Department of Pediatrics Orthopedics and Traumatology, University of Medical Sciences, Poznan, Poland.
Front Neurol. 2021 Mar 18;12:635894. doi: 10.3389/fneur.2021.635894. eCollection 2021.
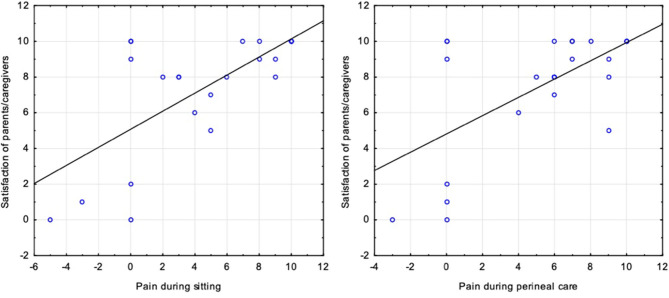
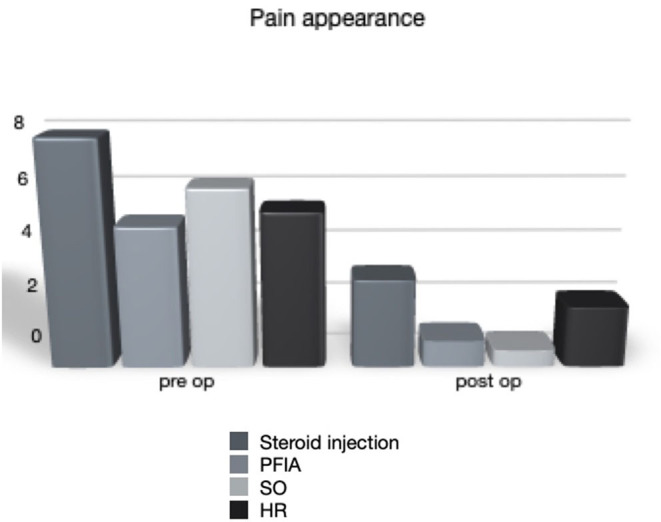
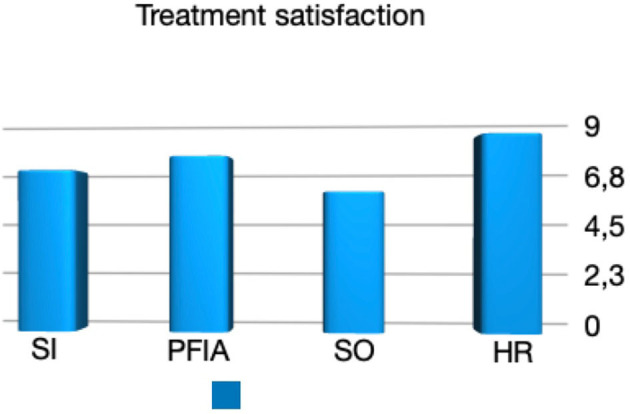
Pain appearance is one the most common complication of spastic hip disease in children with cerebral palsy (CP). It determines child and caregiver quality of life and life priorities. Reconstruction hip surgery should be considered as a treatment of choice. Some clinical conditions give the inability to perform such a procedure. In our paper, we would like to present four palliative methods of spastic hip dislocation treatment in children with CP. We analyzed four groups of patients treated because of hip pain. Inclusion criteria were pain appearance (visual analog scale-11 or numeric rating scale-11) and hip joint dislocation (migration percentage >80%). All patients were admitted to our department between 2008 and 2018. In the first group, patients were treated only by steroid injections to hip joints; in the second group, patients were recruits after hip interposition arthroplasty with shoulder spacer; in the third group, they were patients after valgus subtrochanteric osteotomy (Schanz); and in the fourth group, these were patients after proximal femoral resection (Castle procedure). The minimal follow-up time was 2 years. The first group consisted of 15 patients (15 hips) with a mean age of 15.5 (8-17) years; the second group, 20 patients (24 hips) with a mean age of 14.2 (9-22.6) years; the third group, 22 patients (24 hips) with a mean age of 13.5 (7-20.5) years; and the fourth group, 10 patients (15 hips) with a mean age of 12.9 (7-17.6) years. Radiological evaluation was based on a standardized anteroposterior X-ray of the hip joints. Pain severity before surgery and at the last follow-up time was measured by visual analog scale-11. Parents or caregivers were asked about their child's pain during sitting, perineal care, and rest. During the visit, all caregivers were asked about treatment satisfaction (no 0 to max 10) and if they would decide again for the same surgery. In all groups of patients, we observed a decrease in pain complaints. The observed reduction of pain in the first group was from 7.88 (4-10) to 3.08 (0-8) ( = 0.05), but results of injection were observed only for 4 months (2-8), and it has to be repeated (average: two times). In the second group, level of pain was reduced from 4.93 (1-10) to 0.93 (0-5) ( < 0.001); in the third group, from 6.22 (3-10) to 0.59 (0-6) ( < 0.001); and in the fourth group, pain reduces from 5.43 (2-10) to 2.13 (0-5) ( < 0.001). Observed changes concerned mostly sitting position and perineal care. The complication rate was in the second group, 6 of 24 cases of extraarticular ossification; in the third group, 2 of 24 cases with extraarticular ossification, two cases of revision surgery. In the fourth group, two cases needed another femoral resection. In the first group, five patients died during follow-up time, so they were excluded from the study. In the steroid injection group, parents' treatment evaluation was 6.83 (0-10), and only in three cases that they would resign from the treatment. In the hip interposition arthroplasty group, caregivers' evaluation was 7.41 (0-10), and in five cases, parents did not accept the surgery. In the Schanz osteotomy group, parents' evaluation was 5.9 (0-10), and in eight cases, caregivers would not repeat surgery. In the proximal femoral resection group, satisfaction was the highest, 8.3 (3-10), and only two parents would not decide for surgery again. All procedures can be considered as palliative treatment options for pain complain in a spastic hip joint dislocation in children with CP. Steroid injections to the hip joint need to be repeated, and with the follow-up time, it becomes less effective. Steroid injection seems to be the treatment of choice for patients with general anesthesia contraindications. Interposition arthroplasty of the hip joint seems to give better final results, but the highest parents' satisfaction surprisingly was observed in the proximal femoral resection group, but differences were not statistically significant.

疼痛表现是脑瘫(CP)患儿痉挛性髋关节疾病最常见的并发症之一。它决定了患儿及其照料者的生活质量和生活重心。髋关节重建手术应被视为首选治疗方法。但某些临床情况使得无法实施该手术。在本文中,我们将介绍四种治疗CP患儿痉挛性髋关节脱位的姑息治疗方法。我们分析了四组因髋关节疼痛接受治疗的患者。纳入标准为出现疼痛(视觉模拟评分-11或数字评定量表-11)以及髋关节脱位(移位百分比>80%)。所有患者均于2008年至2018年期间入住我科。第一组患者仅接受髋关节类固醇注射治疗;第二组患者在进行髋关节间置关节成形术并使用肩部间隔物后纳入研究;第三组患者接受股骨转子下外翻截骨术(尚茨截骨术);第四组患者接受股骨近端切除术(卡斯尔手术)。最短随访时间为2年。第一组由15例患者(15个髋关节)组成,平均年龄为15.5(8 - 17)岁;第二组有20例患者(24个髋关节),平均年龄为14.2(9 - 22.6)岁;第三组有22例患者(24个髋关节),平均年龄为13.5(7 - 20.5)岁;第四组有10例患者(15个髋关节),平均年龄为12.9(7 - 17.6)岁。影像学评估基于标准化的髋关节前后位X线片。术前及最后随访时的疼痛严重程度通过视觉模拟评分-11进行测量。询问父母或照料者孩子在坐立、会阴护理及休息时的疼痛情况。在就诊时,询问所有照料者对治疗的满意度(0分为不满意至10分为非常满意)以及他们是否会再次选择相同的手术。在所有患者组中,我们观察到疼痛主诉有所减少。第一组观察到的疼痛减轻情况是从7.88(4 - 10)降至3.08(0 - 8)(P = 0.05),但注射效果仅观察到4个月(2 - 8个月),且必须重复注射(平均:两次)。第二组疼痛程度从4.93(1 - 10)降至0.93(0 - 5)(P < 0.001);第三组从6.22(3 - 10)降至0.59(0 - 6)(P < 0.001);第四组疼痛从5.43(2 - 10)降至2.13(0 - 5)(P < 0.001)。观察到的变化主要涉及坐姿和会阴护理。并发症发生率方面,第二组24例中有6例发生关节外骨化;第三组24例中有2例发生关节外骨化,2例需要翻修手术。第四组有2例需要再次进行股骨切除术。第一组中有5例患者在随访期间死亡,因此被排除在研究之外。在类固醇注射组中,父母对治疗的评价为6.83(0 - 10),只有3例父母表示会放弃治疗。在髋关节间置关节成形术组中,照料者的评价为7.41(0 - 10),有5例父母不接受该手术。在尚茨截骨术组中,父母的评价为5.9(来0 - 10),有8例照料者不会再次选择该手术。在股骨近端切除术组中,满意度最高,为8.3(3 - 10),只有2例父母不会再次选择该手术。所有这些手术方法都可被视为治疗CP患儿痉挛性髋关节脱位疼痛主诉的姑息治疗选择。髋关节类固醇注射需要重复进行,且随着随访时间推移,效果会变差。类固醇注射似乎是有全身麻醉禁忌证患者的首选治疗方法。髋关节间置关节成形术似乎能取得更好的最终效果,但令人惊讶的是,股骨近端切除术组父母的满意度最高,但差异无统计学意义。