Department of Radiation Oncology, Guangxi Medical University Cancer Hospital, Nanning, 530001, Guangxi Zhuang Autonomous Region, China.
Department of Radiation Oncology, Rui Kang Hospital, Guangxi Traditional Chinese Medical University, Nanning, 530001, Guangxi Zhuang Autonomous Region, China.
Radiat Oncol. 2021 Apr 21;16(1):79. doi: 10.1186/s13014-021-01778-6.
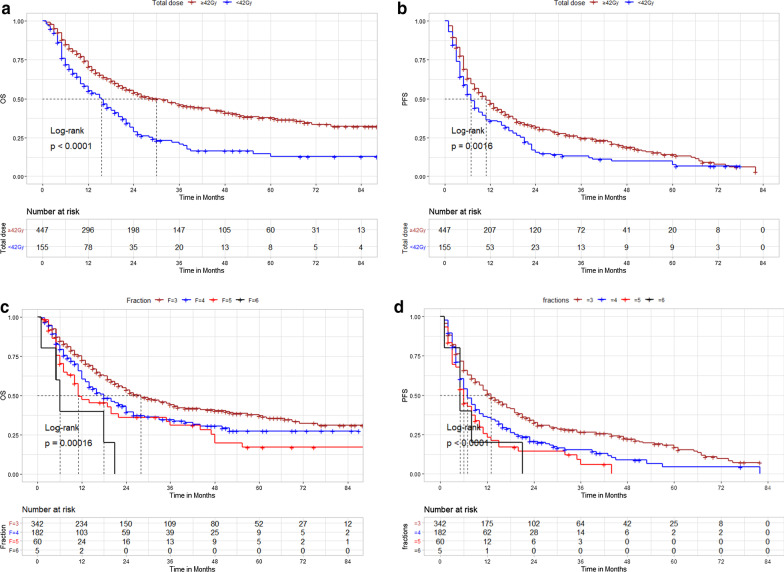
The optimal dose and fractionation scheme of stereotactic body radiation therapy (SBRT) for hepatocellular carcinoma (HCC) remains unclear due to different tolerated liver volumes and degrees of cirrhosis. In this study, we aimed to verify the dose-survival relationship to optimize dose selection for treatment of HCC.
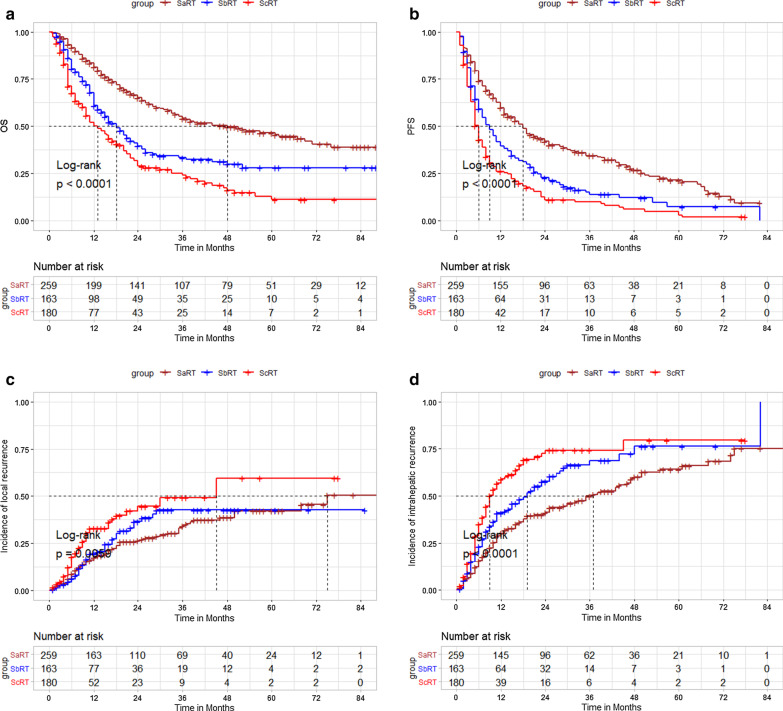
This multicenter retrospective study included 602 patients with HCC, treated with SBRT between January 2011 and March 2017. The SBRT dosage was classified into high dose, moderate dose, and low dose levels: SaRT (BED ≥ 100 Gy), SbRT (EQD > 74 Gy to BED < 100 Gy), and ScRT (EQD < 74 Gy). Overall survival (OS), progression-free survival (PFS), local control (LC), and intrahepatic control (IC) were evaluated in univariable and multivariable analyses.
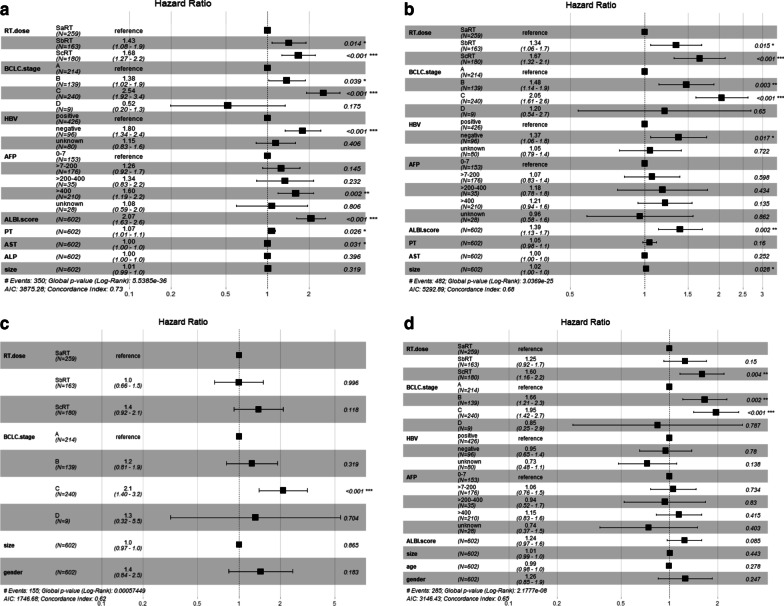
The median tumor size was 5.6 cm (interquartile range [IQR] 1.1-21.0 cm). The median follow-up time was 50.0 months (IQR 6-100 months). High radiotherapy dose correlated with better outcomes. After classifying into the SaRT, SbRT, and ScRT groups, three notably different curves were obtained for long-term post-SBRT survival and intrahepatic control. On multivariate analysis, higher radiation dose was associated with improved OS, PFS, and intrahepatic control.
If tolerated by normal tissue, we recommend SaRT (BED ≥ 100 Gy) as a first-line ablative dose or SbRT (EQD ≥ 74 Gy) as a second-line radical dose. Otherwise, ScRT (EQD < 74 Gy) is recommended as palliative irradiation.
由于不同的耐受肝体积和肝硬化程度,立体定向体放射治疗(SBRT)治疗肝细胞癌(HCC)的最佳剂量和分割方案仍不清楚。在这项研究中,我们旨在验证剂量-生存关系,以优化 HCC 的治疗剂量选择。
这项多中心回顾性研究纳入了 2011 年 1 月至 2017 年 3 月接受 SBRT 治疗的 602 例 HCC 患者。SBRT 剂量分为高剂量、中剂量和低剂量水平:SaRT(BED≥100Gy)、SbRT(EQD>74Gy 至 BED<100Gy)和 ScRT(EQD<74Gy)。在单变量和多变量分析中评估了总生存期(OS)、无进展生存期(PFS)、局部控制率(LC)和肝内控制率(IC)。
肿瘤大小的中位数为 5.6cm(四分位距[IQR]1.1-21.0cm)。中位随访时间为 50.0 个月(IQR6-100 个月)。高放疗剂量与更好的结果相关。在将患者分为 SaRT、SbRT 和 ScRT 组后,获得了三条明显不同的 SBRT 后长期生存和肝内控制曲线。多变量分析显示,较高的放疗剂量与 OS、PFS 和肝内控制的改善相关。
如果正常组织可耐受,我们建议将 SaRT(BED≥100Gy)作为一线消融剂量,或将 SbRT(EQD≥74Gy)作为二线根治性剂量。否则,建议使用 ScRT(EQD<74Gy)作为姑息性照射。