Cancer Genetics Lab, Pulmonary Medicine Division, Department of Medicine, Brigham and Women's Hospital and Harvard Medical School, Boston, Massachusetts, United States of America.
Department of Cancer Biology, Dana-Farber Cancer Institute, Department of Biological Chemistry and Molecular Pharmacology, Harvard Medical School, Boston, Massachusetts, United States of America.
PLoS One. 2021 Apr 23;16(4):e0248380. doi: 10.1371/journal.pone.0248380. eCollection 2021.
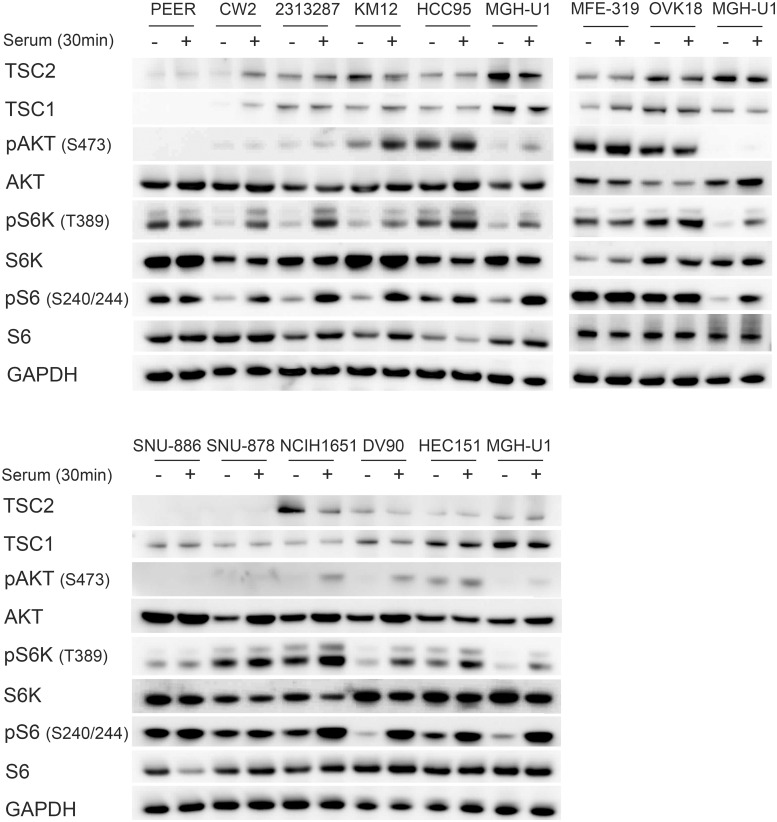
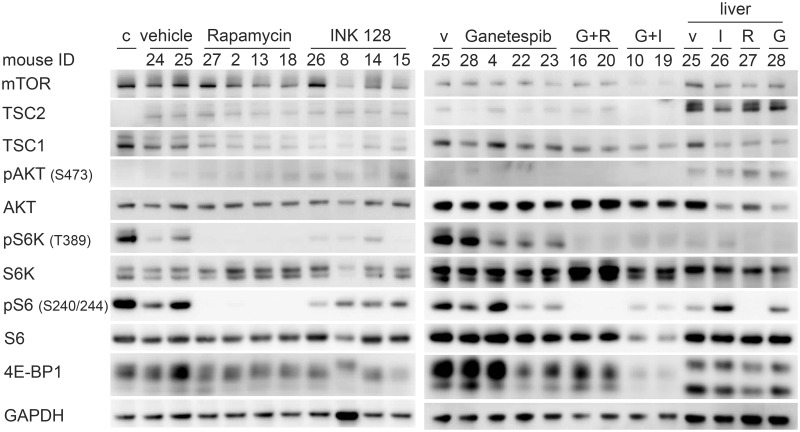
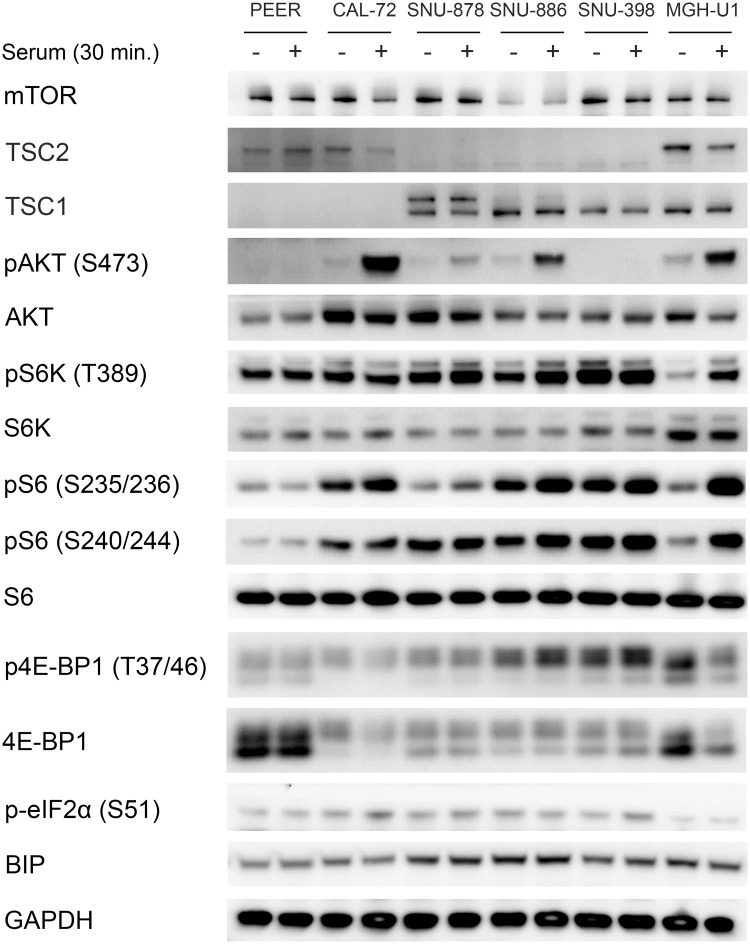
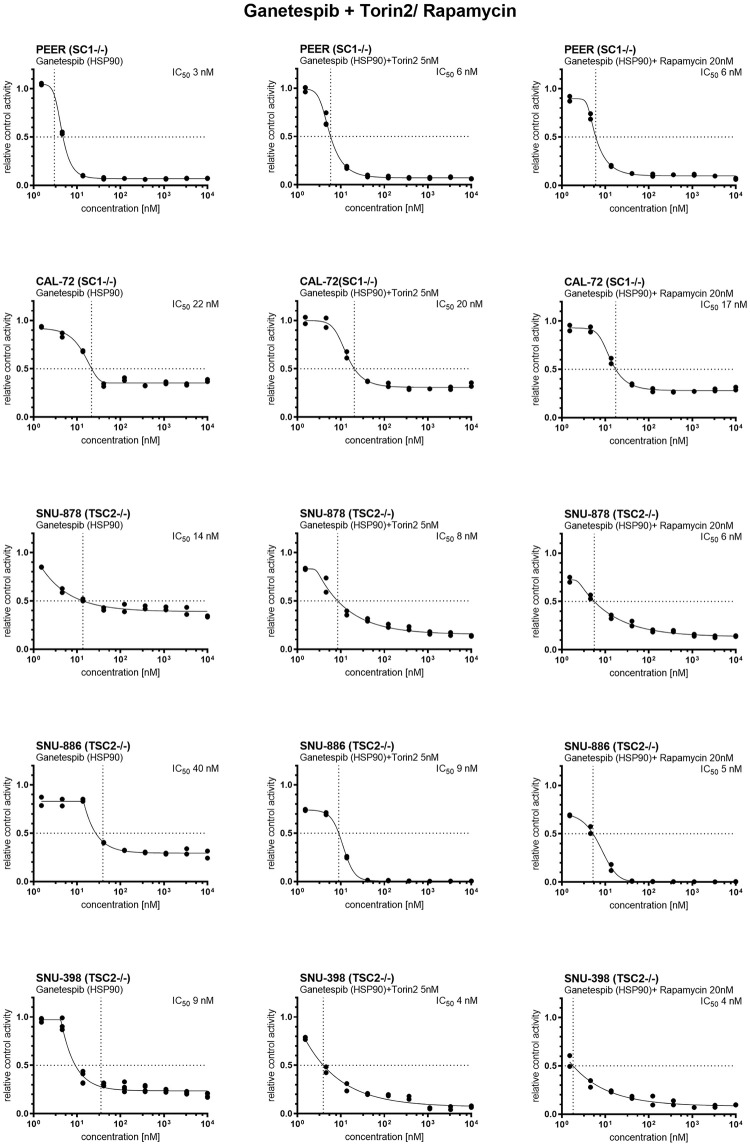
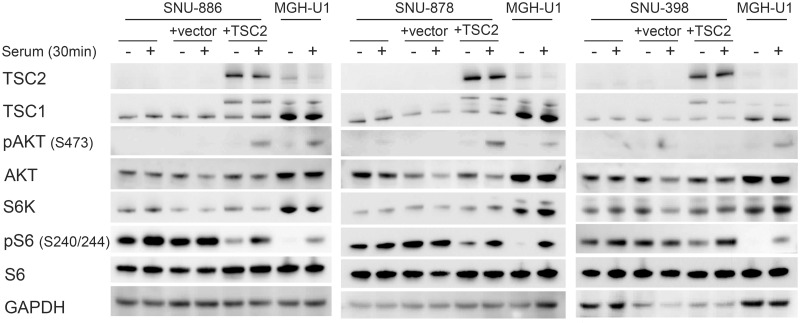
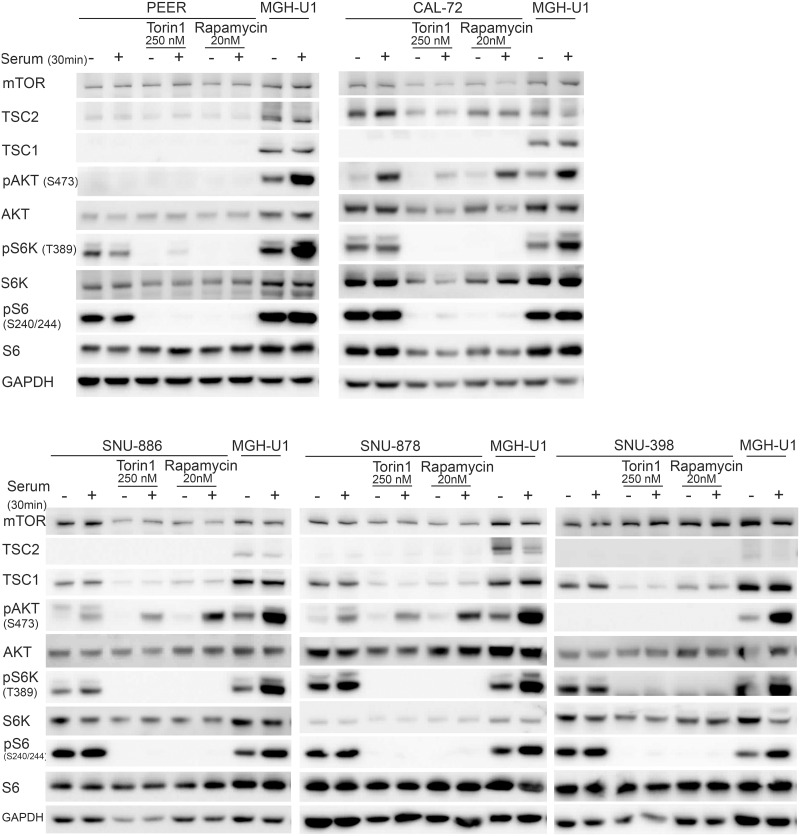
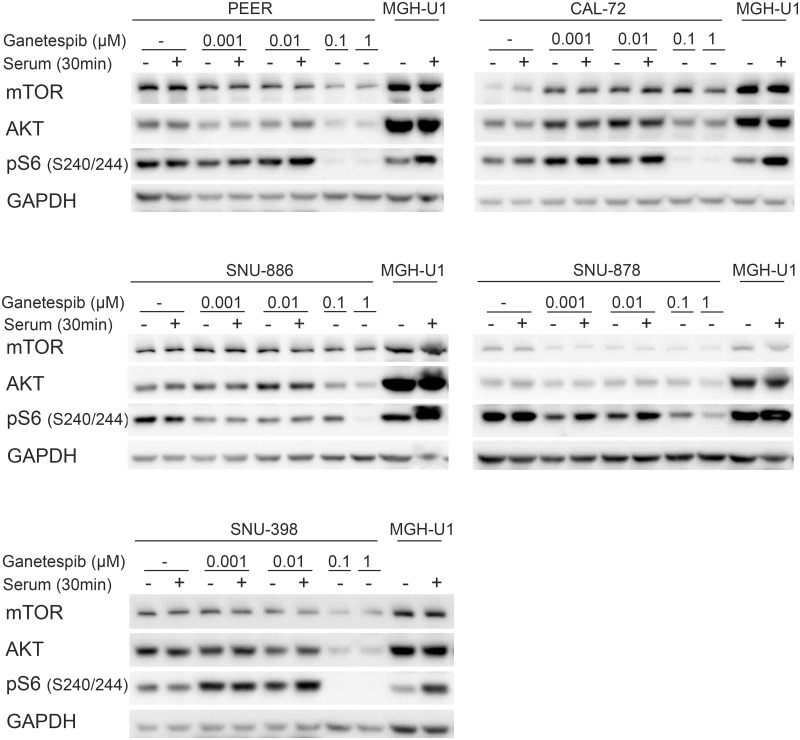
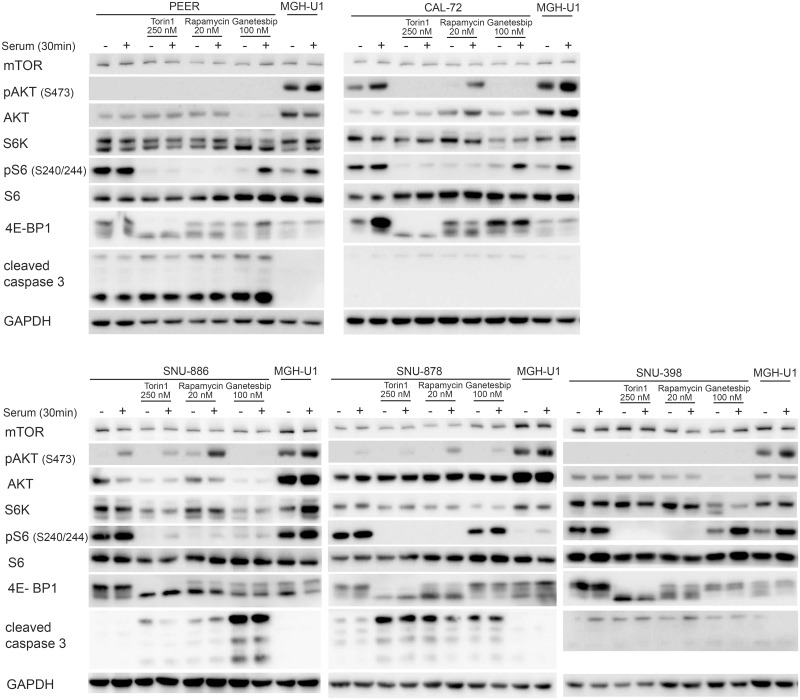
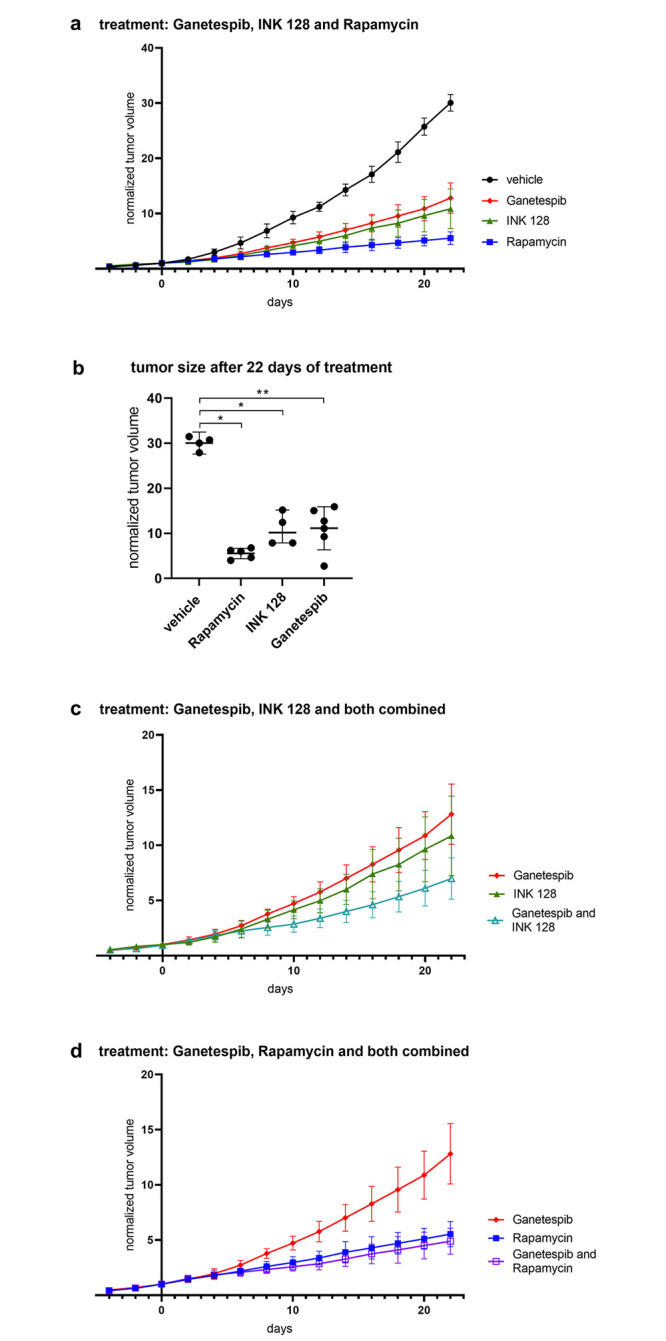
Inactivating mutations in either TSC1 or TSC2 cause Tuberous Sclerosis Complex, an autosomal dominant disorder, characterized by multi-system tumor and hamartoma development. Mutation and loss of function of TSC1 and/or TSC2 also occur in a variety of sporadic cancers, and rapamycin and related drugs show highly variable treatment benefit in patients with such cancers. The TSC1 and TSC2 proteins function in a complex that inhibits mTORC1, a key regulator of cell growth, which acts to enhance anabolic biosynthetic pathways. In this study, we identified and validated five cancer cell lines with TSC1 or TSC2 mutations and performed a kinase inhibitor drug screen with 197 compounds. The five cell lines were sensitive to several mTOR inhibitors, and cell cycle kinase and HSP90 kinase inhibitors. The IC50 for Torin1 and INK128, both mTOR kinase inhibitors, was significantly increased in three TSC2 null cell lines in which TSC2 expression was restored. Rapamycin was significantly more effective than either INK128 or ganetespib (an HSP90 inhibitor) in reducing the growth of TSC2 null SNU-398 cells in a xenograft model. Combination ganetespib-rapamycin showed no significant enhancement of growth suppression over rapamycin. Hence, although HSP90 inhibitors show strong inhibition of TSC1/TSC2 null cell line growth in vitro, ganetespib showed little benefit at standard dosage in vivo. In contrast, rapamycin which showed very modest growth inhibition in vitro was the best agent for in vivo treatment, but did not cause tumor regression, only growth delay.
在 TSC1 或 TSC2 中发生失活突变会导致结节性硬化症,这是一种常染色体显性遗传疾病,其特征是多系统肿瘤和错构瘤的发展。TSC1 和/或 TSC2 的突变和功能丧失也发生在各种散发性癌症中,雷帕霉素和相关药物在患有此类癌症的患者中显示出高度可变的治疗益处。TSC1 和 TSC2 蛋白在抑制 mTORC1 的复合物中发挥作用,mTORC1 是细胞生长的关键调节剂,它作用于增强合成代谢生物合成途径。在这项研究中,我们鉴定并验证了具有 TSC1 或 TSC2 突变的五种癌细胞系,并对 197 种化合物进行了激酶抑制剂药物筛选。这五种细胞系对几种 mTOR 抑制剂以及细胞周期激酶和 HSP90 激酶抑制剂敏感。在 TSC2 缺失的三种细胞系中,当恢复 TSC2 表达时,Torin1 和 INK128 的 IC50(两种 mTOR 激酶抑制剂)均显著增加。在异种移植模型中,雷帕霉素在降低 TSC2 缺失的 SNU-398 细胞生长方面比 INK128 或 ganetespib(HSP90 抑制剂)更有效。Ganetespib-雷帕霉素联合用药对抑制生长的作用没有明显增强作用。因此,尽管 HSP90 抑制剂在体外对 TSC1/TSC2 缺失细胞系的生长具有很强的抑制作用,但 ganetespib 在体内标准剂量下几乎没有获益。相比之下,雷帕霉素在体外显示出非常温和的生长抑制作用,是体内治疗的最佳药物,但不会导致肿瘤消退,只能延迟生长。