Wetwittayakhlang Panu, Rujeerapaiboon Natthapat, Wetwittayakhlung Poowadon, Sripongpun Pimsiri, Pruphetkaew Nannapat, Jandee Sawangpong, Chamroonkul Naichaya, Piratvisuth Teerha
Gastroenterology and Hepatology Unit, Division of Internal Medicine, Faculty of Medicine, Prince of Songkla University, Songkhla 90110, Thailand.
Division of Pathology, Faculty of Medicine, Prince of Songkla University, Songkhla 90110, Thailand.
Gastroenterol Res Pract. 2021 Apr 6;2021:8886525. doi: 10.1155/2021/8886525. eCollection 2021.
Tissue-invasive gastrointestinal cytomegalovirus (TI-GI CMV) disease is common in immunocompromised patients, but the increasing prevalence in immunocompetent patients has been reported. This study compared the clinical manifestations, endoscopic features, treatment outcomes, and predictors for inhospital mortality of TI-GI CMV between immunocompromised and immunocompetent patients.
Patients with HIV infection, malignancy, or receiving immunosuppressive agents (chemotherapy, high dose, or long-term corticosteroids) were defined as the immunocompromised group. Demographic and inhospital mortality data were obtained and retrospectively analyzed.
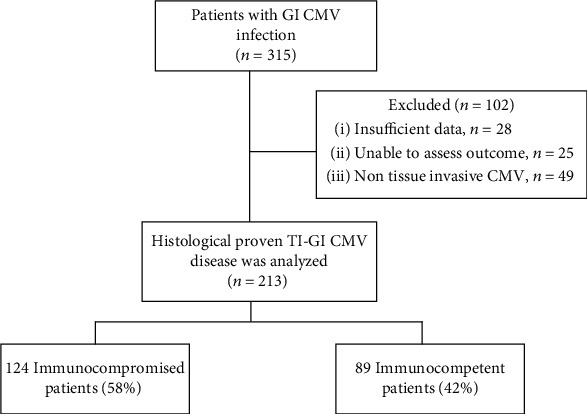
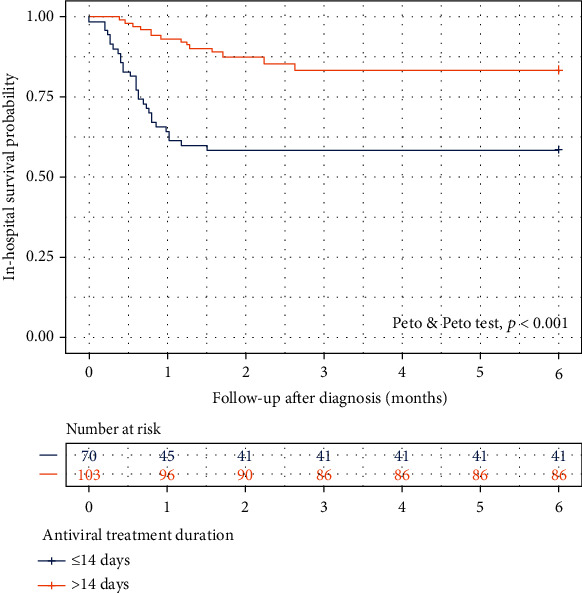
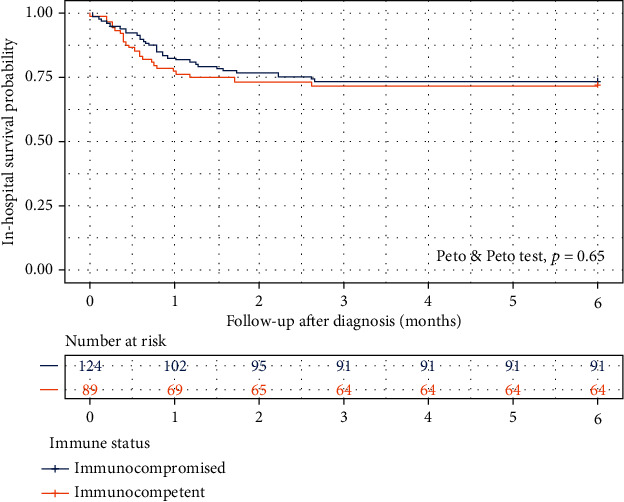
A total of 213 patients (89 immunocompetent) with histologically confirmed TI-GI CMV were enrolled. Immunocompetent patients were older (70 vs. 52 years; < 0.001), had more GI bleeding as a presenting symptom (47.2% vs. 29.0%; = 0.010), and shorter symptom onset (2 vs. 14 days, = 0.018). Concomitant extra-GI involvement was only seen in the immunocompromised group (6.5% vs. 0%; = 0.02). Diffuse GI tract (14.5% vs. 4.5%; = 0.032) and esophageal involvement (14.5% vs. 5.6%; = 0.046) were more frequent in the immunocompromised, while small bowel involvement was more frequent in the immunocompetent group (19.1% vs. 8.1%; = 0.029). An overall inhospital mortality was 27.7%. There was no significant difference in inhospital survival probability between the two groups (Peto-Peto test, = 0.65). ICU admission (hazard ratio [HR] 7.21; 95% CI 2.55-20.36), sepsis or shock (HR 1.98; 95% CI 1.08-3.66), malnutrition (HR 2.62; 95% CI 1.05-7.01), and receiving chemotherapy (HR 5.2; 95% CI 1.89-14.29) were independent factors for inhospital mortality. Antiviral treatment for more than 14 days was the only protective factor to improve survival (Peto-Peto test, < 0.001).
Immunocompetent and immunocompromised patients with TI-GI CMV disease had distinct clinical and endoscopic characteristics. There was no significant difference in the inhospital mortality between the two groups. The factors for mortality were ICU admission, sepsis/shock, malnutrition, and receiving chemotherapy. Early diagnosis and initiation of antiviral treatment might improve the survival probability.
组织侵袭性胃肠道巨细胞病毒(TI-GI CMV)疾病在免疫功能低下患者中很常见,但有报道称其在免疫功能正常患者中的患病率也在增加。本研究比较了免疫功能低下和免疫功能正常患者TI-GI CMV的临床表现、内镜特征、治疗结果及住院死亡率的预测因素。
将感染HIV、患有恶性肿瘤或接受免疫抑制剂治疗(化疗、高剂量或长期使用皮质类固醇)的患者定义为免疫功能低下组。获取人口统计学和住院死亡率数据并进行回顾性分析。
共纳入213例经组织学确诊为TI-GI CMV的患者(89例免疫功能正常)。免疫功能正常患者年龄较大(70岁对52岁;P<0.001),以胃肠道出血为首发症状的比例更高(47.2%对29.0%;P=0.010),症状出现时间更短(2天对14天,P=0.018)。仅在免疫功能低下组中观察到合并胃肠道外受累(6.5%对0%;P=0.02)。免疫功能低下患者弥漫性胃肠道受累(14.5%对4.5%;P=0.032)和食管受累(14.5%对5.6%;P=0.046)更为常见,而免疫功能正常组小肠受累更为常见(19.1%对8.1%;P=0.029)。总体住院死亡率为27.7%。两组间住院生存概率无显著差异(Peto-Peto检验,P=0.65)。入住重症监护病房(风险比[HR]7.21;95%置信区间2.55-20.36)、脓毒症或休克(HR 1.98;95%置信区间1.08-3.66)、营养不良(HR 2.62;95%置信区间1.05-7.01)以及接受化疗(HR 5.2;95%置信区间1.89-14.29)是住院死亡率的独立因素。抗病毒治疗超过1天是改善生存的唯一保护因素(Peto-Peto检验,P<0.001)。
TI-GI CMV疾病的免疫功能正常和免疫功能低下患者具有不同的临床和内镜特征。两组间住院死亡率无显著差异。死亡因素包括入住重症监护病房、脓毒症/休克、营养不良和接受化疗。早期诊断和启动抗病毒治疗可能提高生存概率。