Faculty of Medicine, University of Novi Sad, Novi Sad, Serbia.
Clinical Centre of Vojvodina, Clinic for Infectious Diseases, Novi Sad, Serbia.
PLoS One. 2021 Apr 30;16(4):e0251010. doi: 10.1371/journal.pone.0251010. eCollection 2021.
We aimed to describe the epidemiology of catheter-related bloodstream infections (CRBSIs) in onco-hematological neutropenic patients during a 25-year study period, to evaluate the risk factors for Gram-negative bacilli (GNB) CRBSI, as well as rates of inappropriate empirical antibiotic treatments (IEAT) and mortality.
MATERIALS/METHODS: All consecutive episodes of CRBSIs were prospectively collected (1994-2018). Changing epidemiology was evaluated comparing five-year time spans. A multivariate regression model was built to evaluate risk factors for GNB CRBSIs.
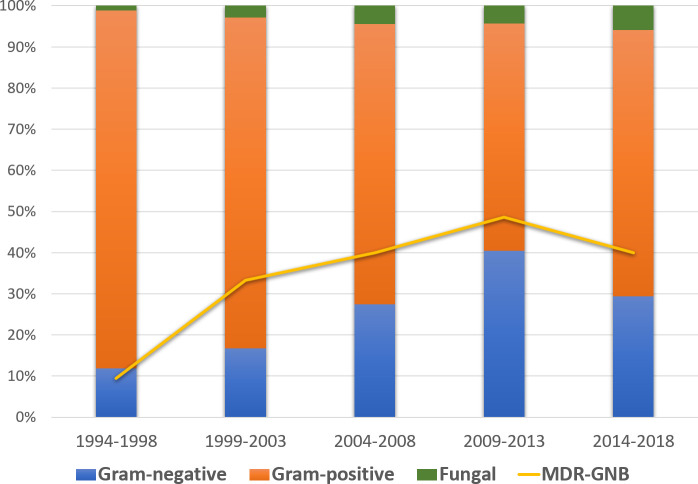
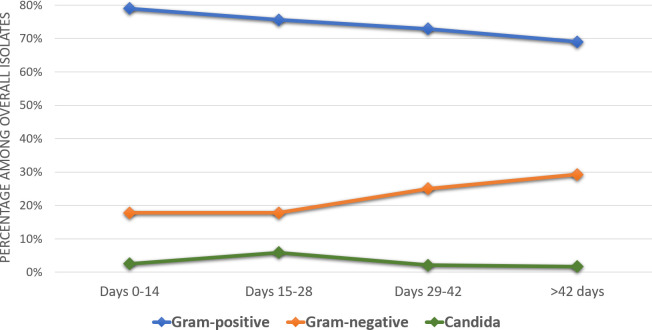
482 monomicrobial CRBSIs were documented. The proportion of CRBSIs among all BSIs decreased over time from 41.2% to 15.8% (p<0.001). CRBSIs epidemiology has been changing: the rate of GNB increased over time (from 11.9% to 29.4%; p<0.001), as well as the absolute number and rate of multidrug-resistant (MDR) GNB (from 9.5% to 40.0%; p = 0.039). P. aeruginosa increased and comprised up to 40% of all GNB. Independent factors related with GNB-CRBSIs were: longer duration of in-situ catheter (OR 1.007; 95%CI 1.004-1.011), older age (OR 1.016; 95%CI 1.001-1.033), prior antibiotic treatment with penicillins (OR 2.716; 95%CI 1.306-5.403), and current antibiotic treatment with glycopeptides (OR 1.931; 95%CI 1.001-3.306). IEATs were administered to 30.7% of patients, with the highest percentage among MDR P. aeruginosa (76.9%) and S. maltophillia (92.9%). Mortality rate was greater among GNB than GPC-CRBSI (14.4% vs 5.4%; p = 0.002), with mortality increasing over time (from 4.5% to 11.2%; p = 0.003).
A significant shift towards GNB-CRBSIs was observed. Secondarily, and coinciding with an increasing number of GNB-MDR infections, mortality increased over time.
我们旨在描述 25 年研究期间,肿瘤血液病中性粒细胞减少患者中导管相关血流感染(CRBSI)的流行病学,评估革兰氏阴性菌(GNB)CRBSI 的危险因素,以及不适当经验性抗生素治疗(IEAT)和死亡率的发生率。
材料/方法:所有连续的 CRBSI 发作均前瞻性收集(1994-2018 年)。通过比较五个五年时间段来评估不断变化的流行病学。建立了多变量回归模型来评估 GNB CRBSI 的危险因素。
记录了 482 例单微生物 CRBSI。CRBSI 在所有 BSI 中的比例随着时间的推移从 41.2%下降到 15.8%(p<0.001)。CRBSI 流行病学一直在变化:GNB 的发生率随着时间的推移而增加(从 11.9%增加到 29.4%;p<0.001),以及多药耐药(MDR)GNB 的绝对数量和发生率(从 9.5%增加到 40.0%;p=0.039)。铜绿假单胞菌增加并占所有 GNB 的 40%。与 GNB-CRBSI 相关的独立因素是:原位导管留置时间较长(OR 1.007;95%CI 1.004-1.011),年龄较大(OR 1.016;95%CI 1.001-1.033),先前使用青霉素类抗生素治疗(OR 2.716;95%CI 1.306-5.403),以及当前使用糖肽类抗生素治疗(OR 1.931;95%CI 1.001-3.306)。IEAT 治疗了 30.7%的患者,其中 MDR 铜绿假单胞菌(76.9%)和嗜麦芽寡养单胞菌(92.9%)的百分比最高。与 GPC-CRBSI 相比,GNB-CRBSI 的死亡率更高(14.4% vs 5.4%;p=0.002),死亡率随着时间的推移而增加(从 4.5%增加到 11.2%;p=0.003)。
观察到 GNB-CRBSI 显著增加。其次,随着 GNB-MDR 感染数量的增加,死亡率随着时间的推移而增加。