Diabetic Foot Unit, University of Rome Tor Vergata, Viale Oxford 81, 00133, Rome, Italy.
Diabetic Foot Unit, Universidad Complutense de Madrid, Madrid, Spain.
Acta Diabetol. 2021 Oct;58(10):1351-1358. doi: 10.1007/s00592-021-01721-x. Epub 2021 May 3.
To investigate the effectiveness of fast-track pathway (FTP) in the management of diabetic foot ulceration (DFU) after 2 years of implementation.
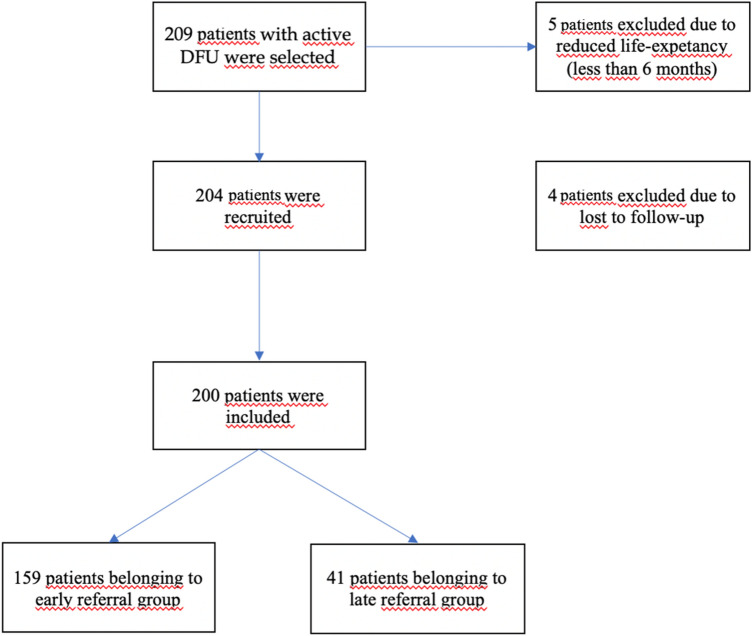
The study group was composed of patients who referred to a specialized DF centre due to DFUs. Those were divided in two groups: early referral (ER) and late referral (LR) patients. According to FTP, ER were considered patients who referred after 2 weeks in the case of uncomplicated non-healing ulcers (superficial, not infected, not ischemic), within 4 days in the case of complicated ulcers (ischemic, deep, mild infection) and within 24 h in the case of severely complicated ulcers (abscess, wet gangrene, fever). Healing, healing time, minor and major amputation, hospitalization, and survival were evaluated. The follow-up was 6 months.
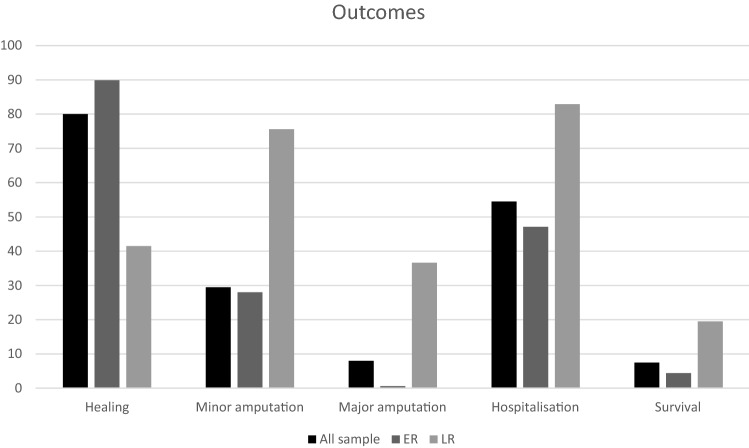
Two hundred patients were recruited. The mean age was 70 ± 13 years, 62.5% were male, 91% were affected by type 2 diabetes with a mean duration of 18 ± 11 years. Within the group, 79.5% had ER while 20.5% had LR. ER patients showed increased rates of healing (89.9 vs. 41.5%, p = 0.001), reduced healing time (10 vs. 16 weeks, p = 0.0002), lower rates of minor (17.6 vs. 75.6%, p < 0.0001) and major amputation (0.6 vs. 36.6%, p < 0.0001), hospitalization (47.1 vs. 82.9%, p = 0.001), and mortality (4.4 vs. 19.5%, p = 0.02) in comparison to LR. At multivariate analysis, ER was an independent predictor of healing, while LR was an independent predictor for minor and major amputation and hospitalization.
After the FTP implementation, less cases of LR were reported in comparison to ER. ER was an independent predictor of positive outcomes such as healing, healing time, limb salvage, hospitalization, and survival.
探讨 2 年后快速通道(FTP)在糖尿病足溃疡(DFU)管理中的效果。
研究组由因 DFU 而到专门 DF 中心就诊的患者组成。这些患者被分为两组:早期转诊(ER)和晚期转诊(LR)患者。根据 FTP,ER 被认为是在无并发症的非愈合性溃疡(浅表、未感染、无缺血)的情况下在 2 周后、在复杂溃疡(缺血、深、轻度感染)的情况下在 4 天内、在严重复杂溃疡(脓肿、湿性坏疽、发热)的情况下在 24 小时内转诊的患者。评估愈合、愈合时间、小截肢和大截肢、住院和存活率。随访 6 个月。
共招募了 200 名患者。平均年龄为 70±13 岁,62.5%为男性,91%患有 2 型糖尿病,平均病程为 18±11 年。在组内,79.5%为 ER,20.5%为 LR。ER 患者的愈合率(89.9% vs. 41.5%,p=0.001)、愈合时间(10 周 vs. 16 周,p=0.0002)、小截肢(17.6% vs. 75.6%,p<0.0001)和大截肢(0.6% vs. 36.6%,p<0.0001)、住院率(47.1% vs. 82.9%,p=0.001)和死亡率(4.4% vs. 19.5%,p=0.02)均低于 LR。多变量分析显示,ER 是愈合的独立预测因子,而 LR 是小截肢和大截肢以及住院的独立预测因子。
FTP 实施后,与 ER 相比,LR 的病例报告减少。ER 是愈合、愈合时间、肢体保存、住院和生存等积极结果的独立预测因子。