West German Study Group, Moenchengladbach, Germany
Breast Center Niederrhein, Bethesda Protestant Hospital Monchengladbach, Monchengladbach, Germany.
J Immunother Cancer. 2021 May;9(5). doi: 10.1136/jitc-2020-002198.
The association of early changes in the immune infiltrate during neoadjuvant chemotherapy (NACT) with pathological complete response (pCR) in triple-negative breast cancer (TNBC) remains unexplored.
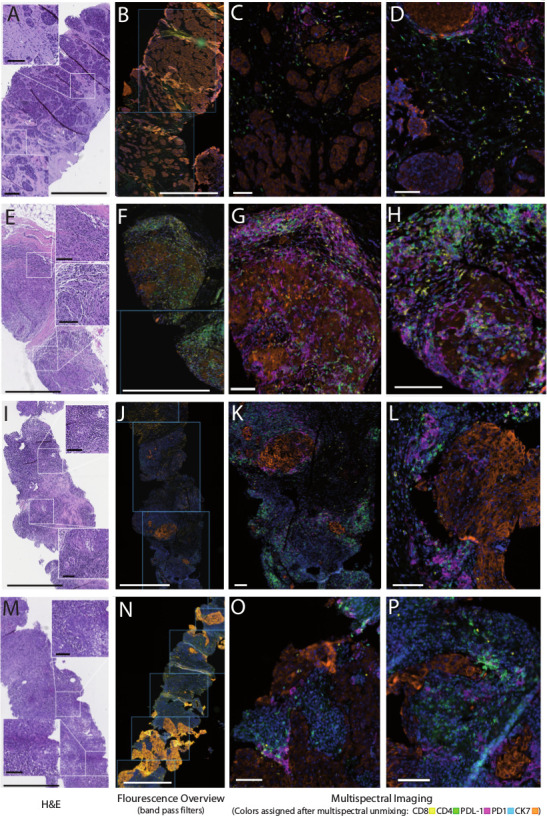
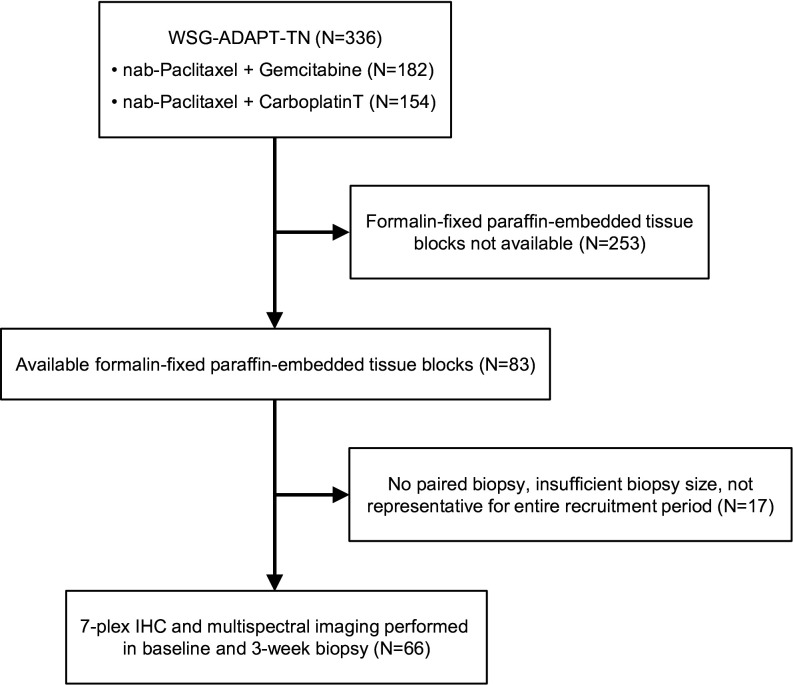
Multiplexed immunohistochemistry was performed in matched tumor biopsies obtained at baseline and after 3 weeks of NACT from 66 patients from the West German Study Group Adjuvant Dynamic Marker-Adjusted Personalized Therapy Trial Optimizing Risk Assessment and Therapy Response Prediction in Early Breast Cancer - Triple Negative Breast Cancer (WSG-ADAPT-TN) trial. Association between CD4, CD8, CD73, T cells, PD1-positive CD4 and CD8 cells, and PDL1 levels in stroma and/or tumor at baseline, week 3 and 3-week change with pCR was evaluated with univariable logistic regression.
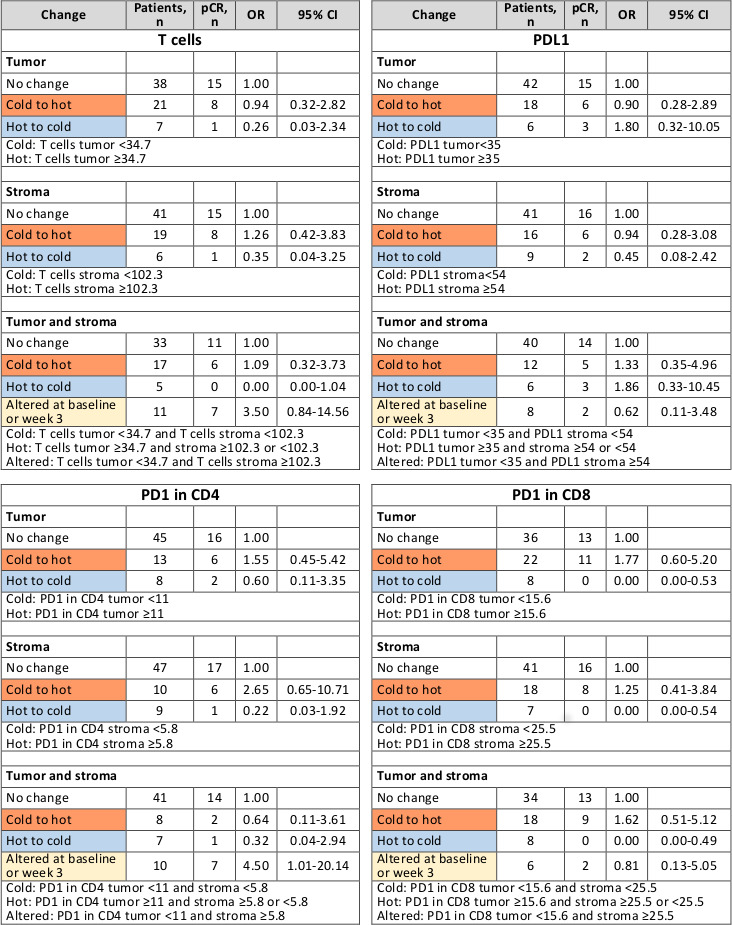
Compared with no change in immune cell composition and functional markers, transition from 'cold' to 'hot' (below-median and above-median marker level at baseline, respectively) suggested higher pCR rates for PD1-positive CD4 (tumor: OR=1.55, 95% CI 0.45 to 5.42; stroma: OR=2.65, 95% CI 0.65 to 10.71) and PD1-positive CD8 infiltrates (tumor: OR=1.77, 95% CI 0.60 to 5.20; stroma: OR=1.25, 95% CI 0.41 to 3.84; tumor+stroma: OR=1.62, 95% CI 0.51 to 5.12). No pCR was observed after 'hot-to-cold' transition in PD1-positive CD8 cells. pCR rates appeared lower after hot-to-cold transitions in T cells (tumor: OR=0.26, 95% CI 0.03 to 2.34; stroma: OR=0.35, 95% CI 0.04 to 3.25; tumor+stroma: OR=0.00, 95% CI 0.00 to 1.04) and PD1-positive CD4 cells (tumor: OR=0.60, 95% CI 0.11 to 3.35; stroma: OR=0.22, 95% CI 0.03 to 1.92; tumor+stroma: OR=0.32, 95% CI 0.04 to 2.94). Higher pCR rates collated with 'altered' distribution (levels below-median and above-median in tumor and stroma, respectively) of T cell (OR=3.50, 95% CI 0.84 to 14.56) and PD1-positive CD4 cells (OR=4.50, 95% CI 1.01 to 20.14).
Our exploratory findings indicate that comprehensive analysis of early immune infiltrate dynamics complements currently investigated predictive markers for pCR and may have a potential to improve guidance for individualized de-escalation/escalation strategies in TNBC.
新辅助化疗(NACT)期间免疫浸润早期变化与三阴性乳腺癌(TNBC)的病理完全缓解(pCR)之间的关联仍未得到探索。
对来自德国西部研究组辅助动态标志物调整个体化治疗试验(WSG-ADAPT-TN)的 66 例患者的基线和 NACT 后 3 周时的匹配肿瘤活检进行了多重免疫组化分析。采用单变量逻辑回归评估基线、第 3 周和 3 周变化时 CD4、CD8、CD73、T 细胞、PD1 阳性 CD4 和 CD8 细胞以及基质和/或肿瘤中 PD-L1 水平与 pCR 的相关性。
与免疫细胞组成和功能标志物无变化相比,从“冷”到“热”(分别为基线时中位数以下和中位数以上的标志物水平)的转变提示 PD1 阳性 CD4(肿瘤:OR=1.55,95%CI 0.45 至 5.42;基质:OR=2.65,95%CI 0.65 至 10.71)和 PD1 阳性 CD8 浸润(肿瘤:OR=1.77,95%CI 0.60 至 5.20;基质:OR=1.25,95%CI 0.41 至 3.84;肿瘤+基质:OR=1.62,95%CI 0.51 至 5.12)的 pCR 率更高。在 PD1 阳性 CD8 细胞从“热”到“冷”的转变后未观察到 pCR。在 T 细胞(肿瘤:OR=0.26,95%CI 0.03 至 2.34;基质:OR=0.35,95%CI 0.04 至 3.25;肿瘤+基质:OR=0.00,95%CI 0.00 至 1.04)和 PD1 阳性 CD4 细胞(肿瘤:OR=0.60,95%CI 0.11 至 3.35;基质:OR=0.22,95%CI 0.03 至 1.92;肿瘤+基质:OR=0.32,95%CI 0.04 至 2.94)从“热”到“冷”的转变后,pCR 率似乎较低。T 细胞(OR=3.50,95%CI 0.84 至 14.56)和 PD1 阳性 CD4 细胞(OR=4.50,95%CI 1.01 至 20.14)的“改变”分布(肿瘤和基质中分别低于中位数和中位数以上的水平)与更高的 pCR 率相关。
我们的探索性发现表明,早期免疫浸润动态的综合分析补充了目前研究的 pCR 预测标志物,可能有潜力改善 TNBC 个体化降阶梯/升阶梯策略的指导。