Department of Chemical Pathology and Metabolic Medicine, St Thomas' Hospital, London, UK.
Metabolic Bone Clinic, Department of Rheumatology, Guy's Hospital, London, UK.
Endocrine. 2021 Sep;73(3):509-529. doi: 10.1007/s12020-021-02735-9. Epub 2021 May 11.
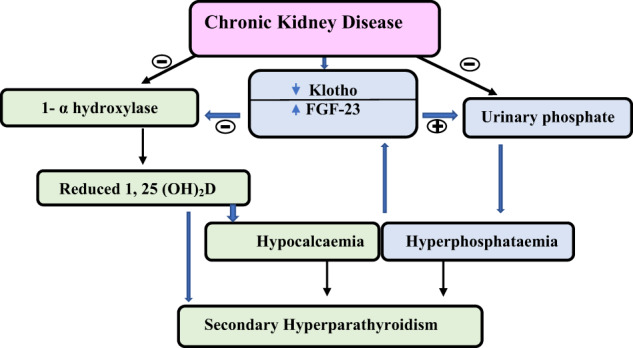
This article aims to review the methods used for the assessment of fracture risk and the use of osteoporosis medications for fracture prevention in the population with CKD, and highlights the difficulties faced by clinicians in the management of these patients and the latest recommendations and guidelines. Chronic kidney disease (CKD) and osteoporosis often co-exist in older adults, and they present a major healthcare challenge. CKD mineral and bone disorder (CKD-MBD) occurs as renal function declines and this syndrome affects most patients in CKD stages 4 and 5. The biochemical abnormalities of CKD-MBD, renal bone disease and risk factors associated with age-related bone loss and osteoporosis lead to a cumulative effect on fracture risk and mortality. There is a need for routine evaluation of fracture risk and fracture prevention in this population. Measurement of bone mineral density (BMD) and the use of the FRAX tool have predictive value for incident fractures in the general population and in CKD. This enables physicians to identify CKD patients most at risk of sustaining a fragility fracture and allows a more targeted approach to fracture prevention. Data analysis from the pivotal trials of therapeutic agents used in osteoporosis show that these drugs can be considered in mild and moderate CKD (stages 1-3 CKD). Off-label drug use in patients with CKD-MBD and more severe renal impairment (CKD stages 4 and 5) could offer significant benefits to sub-groups of patients when carefully tailored to each individual's bone turnover and calcium and phosphate balance. However, this requires a selective approach and treatment decisions based on inference from pathophysiology while we await further trials. Guidelines advocate the correction and/or reduction of the biochemical abnormalities of CKD-MBD before initiation of treatment with osteoporosis drugs and close monitoring during treatment.
本文旨在回顾用于评估 CKD 人群骨折风险和预防骨质疏松症药物的方法,并强调临床医生在管理这些患者时面临的困难以及最新的建议和指南。慢性肾脏病(CKD)和骨质疏松症在老年人中常同时存在,是一个主要的医疗保健挑战。随着肾功能下降,CKD 矿物质和骨代谢紊乱(CKD-MBD)发生,该综合征影响 CKD 4 期和 5 期的大多数患者。CKD-MBD 的生化异常、肾性骨病以及与年龄相关的骨丢失和骨质疏松症相关的危险因素导致骨折风险和死亡率的累积效应。需要对该人群进行常规的骨折风险评估和预防。骨密度(BMD)测量和 FRAX 工具的使用对普通人群和 CKD 患者的骨折事件具有预测价值。这使医生能够识别出最易发生脆性骨折的 CKD 患者,并允许更有针对性地预防骨折。用于骨质疏松症治疗药物的关键试验数据分析表明,在轻度和中度 CKD(CKD 1-3 期)中可以考虑这些药物。在 CKD-MBD 和更严重的肾功能不全(CKD 4 期和 5 期)患者中使用未经批准的药物,当根据个体的骨转换和钙磷平衡进行个体化调整时,可能会为亚组患者带来显著获益。然而,这需要采用选择性方法,并且在等待进一步试验的同时,根据病理生理学推断做出治疗决策。指南主张在开始使用骨质疏松症药物治疗之前纠正和/或减少 CKD-MBD 的生化异常,并在治疗期间密切监测。