Department of Emergency Medicine, University of Michigan, Ann Arbor, MI, USA.
Department of Emergency Medicine, Ascension St. John Hospital, Detroit, MI, USA.
Am J Emerg Med. 2021 Sep;47:267-273. doi: 10.1016/j.ajem.2021.05.005. Epub 2021 May 6.
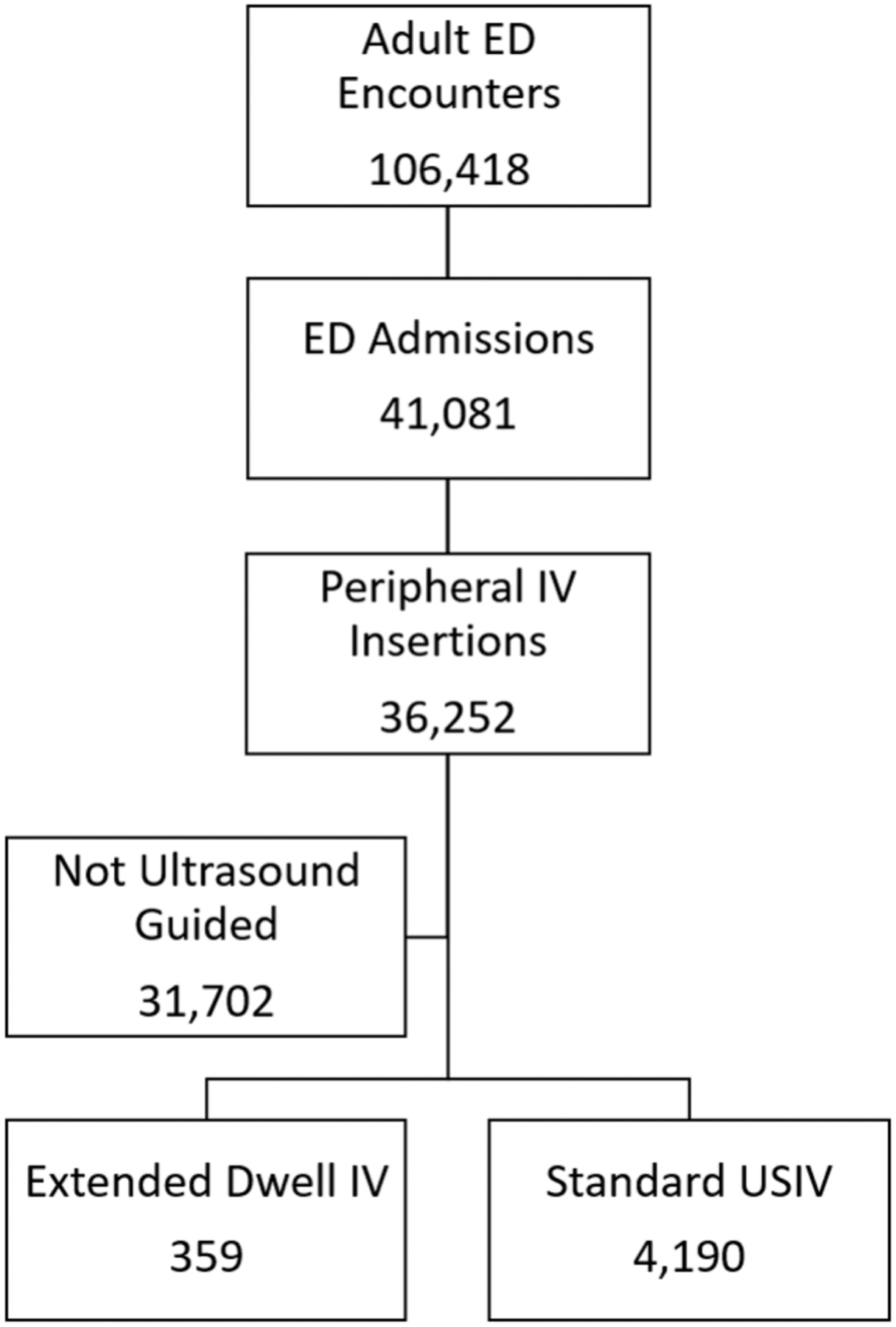
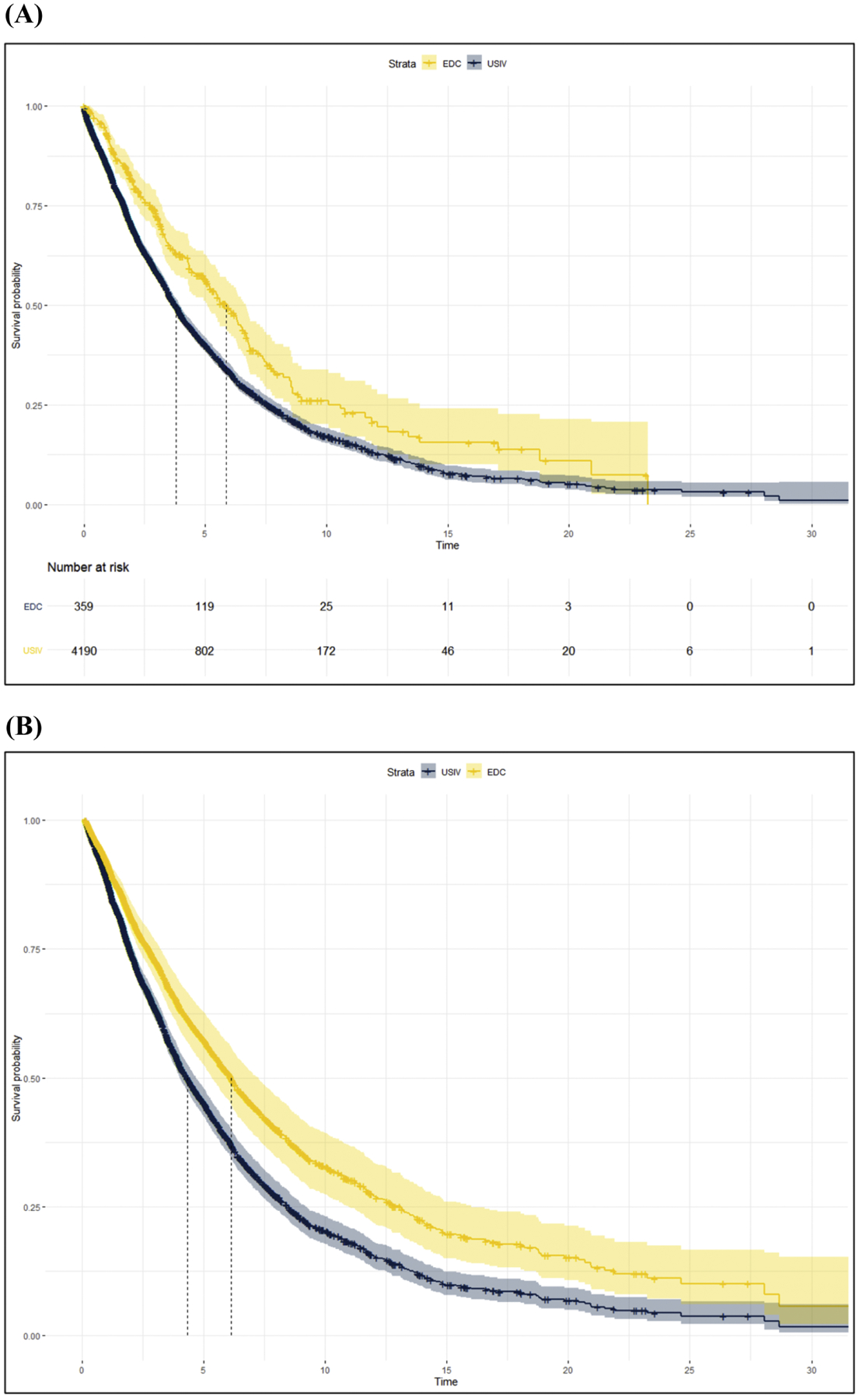
Background Vascular access is a critical component of emergency department (ED) care. Ultrasound guided placement of peripheral intravenous (USIV) catheters is increasingly common. However, USIV are thought to suffer from reduced durability and higher complication rates. Extended dwell catheters (EDC) are long peripheral IVs placed under combined ultrasound and wire guidance. The goal of this study is to compare dwell times and complication rates of EDC to standard peripheral USIV. Methods We performed a retrospective cohort study at a tertiary care adult ED comparing IV placements during a 17-month period (8/1/2018-12/31/2019), stratified by standard USIV versus EDC. The primary outcome was catheter dwell time and secondary outcomes included need for inpatient vascular access team (VAST) consultation, peripherally inserted central catheter (PICC) insertions, and radiocontrast extravasations. Multivariable Cox regression time-to-event analyses were used to evaluate dwell times, adjusting for age, gender, BMI and end-stage renal disease. Results 359 EDC and 4190 standard USIV were included for analysis. Most USIV (95.6%) and EDC (98.3%) were placed by ED technicians trained in ultrasound vascular access. EDC median dwell time (5.9 days [95%CI: 5.1-6.7]) exceeded standard USIV (3.8 days [95% CI: 3.6-4.0]). Patients with EDC placed in the ED required less VAST consultation (0.84 vs 0.99 charges/encounter), had similar rates of PICC line use (8.0% vs 8.4% of encounters) and had no radiocontrast extravasation events. Multivariable Cox regression demonstrated survival benefit (longer dwell time) favoring EDC (HR 0.70 [95%CI 0.60-0.81]). Conclusion Use of EDC results in longer dwell time and reduces subsequent use of vascular access resources, while maintaining low complication rates. EDC demonstrate superior durability which may justify their selection over standard USIV in some patients.
背景 血管通路是急诊科(ED)护理的关键组成部分。超声引导下外周静脉置管(USIV)越来越常见。然而,USIV 被认为耐用性降低,并发症发生率更高。延长留置导管(EDC)是在超声和导丝引导下放置的长外周静脉 IV。本研究的目的是比较 EDC 与标准外周 USIV 的留置时间和并发症发生率。
方法 我们在一家三级成人 ED 进行了回顾性队列研究,比较了 17 个月期间(2018 年 8 月 1 日-2019 年 12 月 31 日)的 IV 置管情况,分为标准 USIV 与 EDC。主要结局是导管留置时间,次要结局包括需要住院血管通路团队(VAST)咨询、经外周插入中心导管(PICC)插入和放射性对比外渗。使用多变量 Cox 回归时间事件分析来评估留置时间,调整年龄、性别、BMI 和终末期肾病。
结果 共纳入 359 例 EDC 和 4190 例标准 USIV 进行分析。大多数 USIV(95.6%)和 EDC(98.3%)均由接受过超声血管通路培训的 ED 技术人员放置。EDC 中位留置时间(5.9 天[95%CI:5.1-6.7])长于标准 USIV(3.8 天[95%CI:3.6-4.0])。ED 中放置 EDC 的患者需要更少的 VAST 咨询(0.84 与 0.99 次就诊费用),使用 PICC 线的比例相似(8.0%与 8.4%的就诊),且无放射性对比外渗事件。多变量 Cox 回归显示 EDC 具有生存优势(留置时间更长)(HR 0.70[95%CI 0.60-0.81])。
结论 使用 EDC 可延长留置时间,并减少随后血管通路资源的使用,同时保持低并发症发生率。EDC 表现出更好的耐用性,在某些患者中,可能证明其优于标准 USIV。