Department of Radiology, Mie University Hospital, 2-174 Edobashi, Tsu, Mie, 514-8507, Japan.
Department of Cardiology and Nephrology, Mie University Hospital, Tsu, Mie, Japan.
J Cardiovasc Magn Reson. 2021 May 17;23(1):56. doi: 10.1186/s12968-021-00749-w.
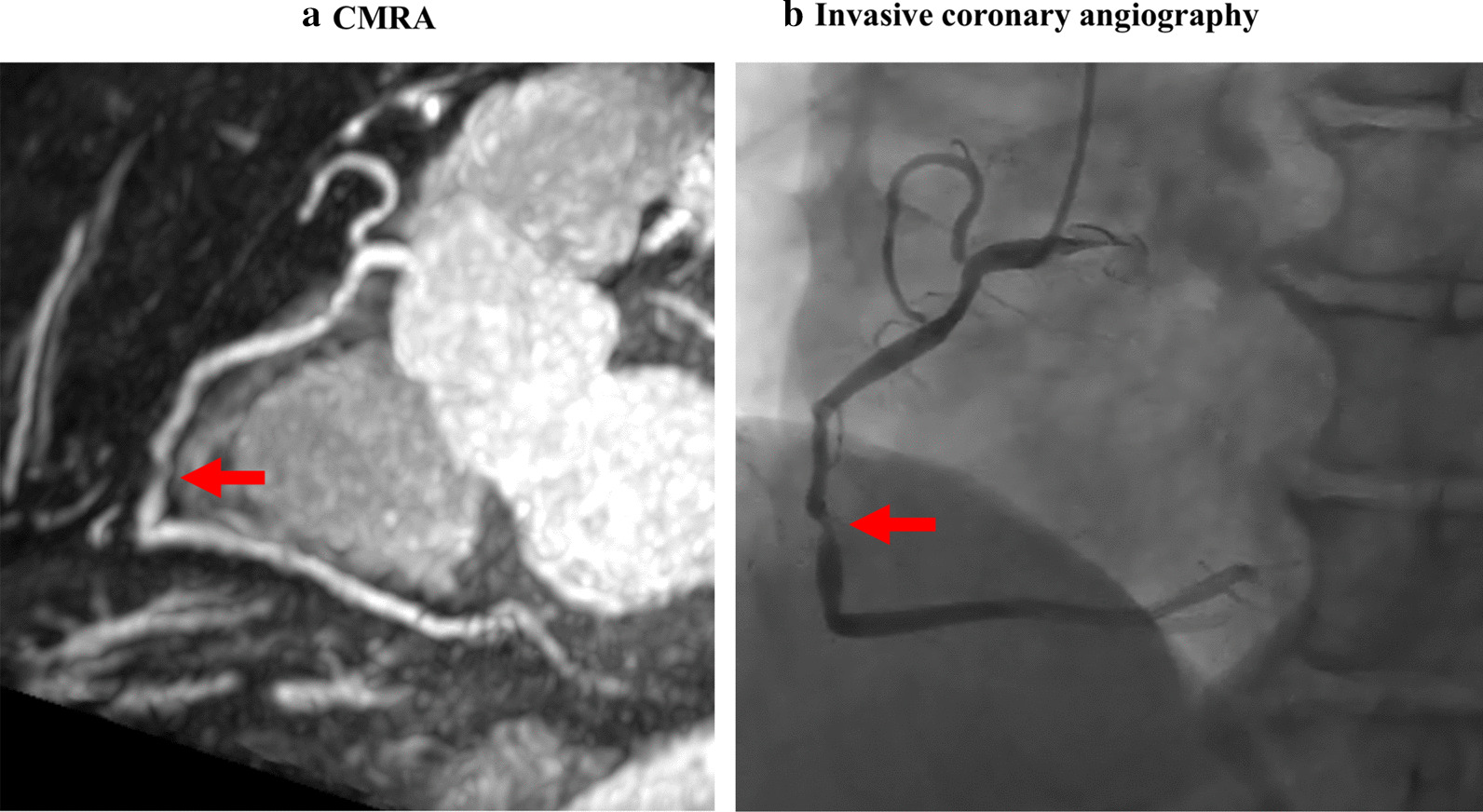
Coronary magnetic resonance angiography (CMRA) allows non-ionizing visualization of luminal narrowing in coronary artery disease (CAD). Although a prior study showed the usefulness of CMRA for risk stratification in short-term follow-up, the long-term prognostic value of CMRA remains unclear. The purpose of this study was to evaluate the long-term prognostic value of CMRA.
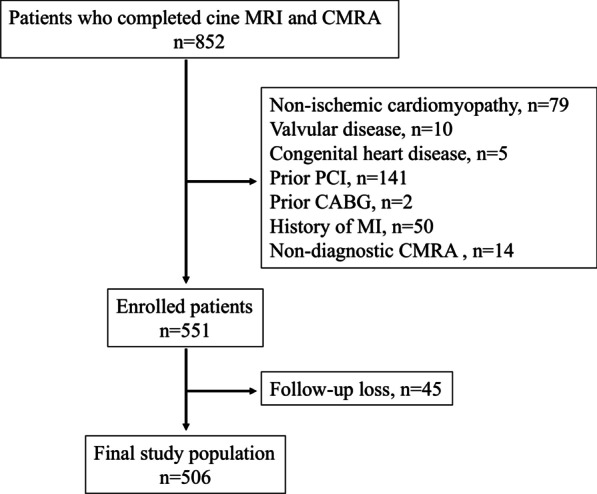
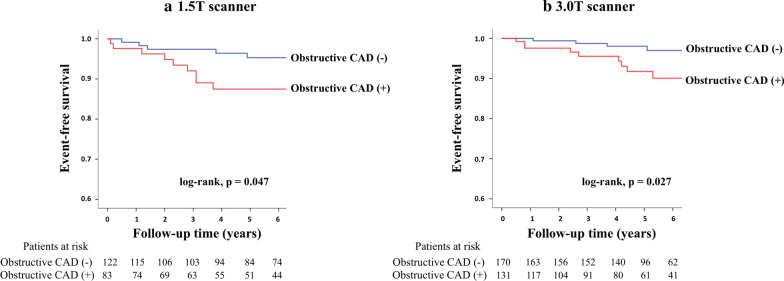
A total of 506 patients without history of myocardial infarction or prior coronary artery revascularization underwent free-breathing whole-heart CMRA between 2009 and 2015. Images were acquired using a 1.5 T or 3 T scanner and visually evaluated as the consensus decisions of two observers. Obstructive CAD on CMRA was defined as luminal narrowing of ≥ 50% in at least one coronary artery. Major adverse cardiac events (MACE) comprised cardiac death, nonfatal myocardial infarction, and unstable angina.
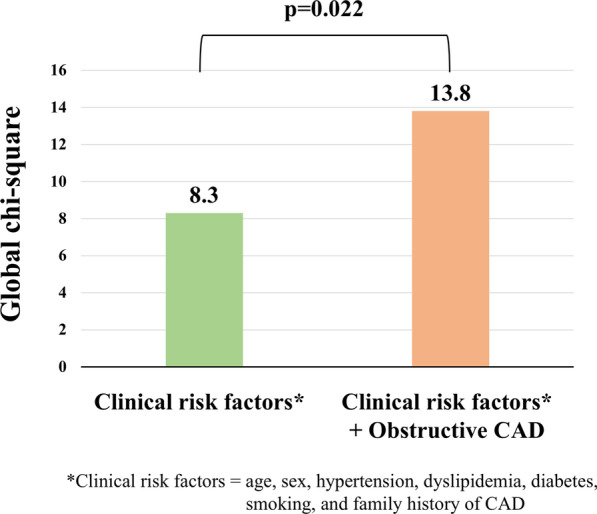
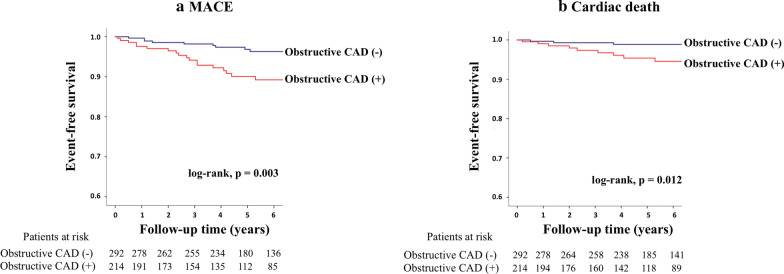
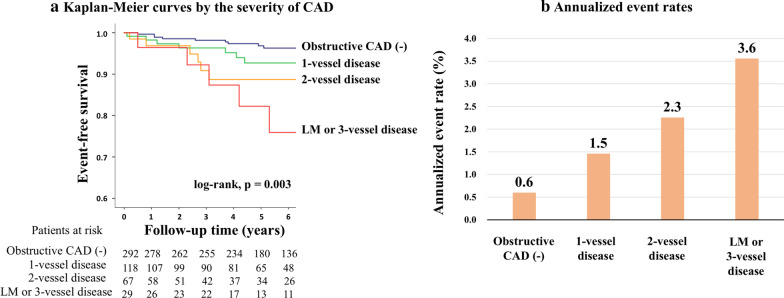
Obstructive CAD on CMRA was observed in 214 patients (42%). During follow-up (median, 5.6 years), 31 MACE occurred. Kaplan-Meier curve analysis revealed a significant difference in event-free survival between patients with and without obstructive CAD for MACE (log-rank, p = 0.003) and cardiac death (p = 0.012). Annualized event rates for MACE in patients with no obstructive CAD, 1-vessel disease, 2-vessel disease, and left-main or 3-vessel disease were 0.6%, 1.5%, 2.3%, and 3.6%, respectively (log-rank, p = 0.003). Cox proportional hazard regression analysis showed that, among obstructive CAD on CMRA and clinical risk factors (age, sex, hypertension, diabetes, dyslipidemia, smoking, and family history of CAD), obstructive CAD and diabetes were significant predictors of MACE (hazard ratios, 2.9 [p = 0.005] and 2.2 [p = 0.034], respectively). In multivariate analysis, obstructive CAD remained an independent predictor (adjusted hazard ratio, 2.6 [p = 0.010]) after adjusting for diabetes. Addition of obstructive CAD to clinical risk factors significantly increased the global chi-square result from 8.3 to 13.8 (p = 0.022).
In long-term follow-up, free breathing whole heart CMRA allows non-invasive risk stratification for MACE and cardiac death and provides incremental prognostic value over conventional risk factors in patients without a history of myocardial infarction or prior coronary artery revascularization. The presence and severity of obstructive CAD detected by CMRA were associated with worse prognosis. Importantly, patients without obstructive CAD on CMRA displayed favorable prognosis.
冠状动脉磁共振血管造影(CMRA)可实现冠状动脉疾病(CAD)管腔狭窄的非电离可视化。尽管先前的研究表明 CMRA 在短期随访中的风险分层具有一定作用,但 CMRA 的长期预后价值仍不清楚。本研究旨在评估 CMRA 的长期预后价值。
2009 年至 2015 年间,共有 506 例无心肌梗死或既往冠状动脉血运重建史的患者接受了自由呼吸式全心 CMRA。使用 1.5T 或 3T 扫描仪进行图像采集,并由两名观察者的共识决策进行视觉评估。CMRA 上的阻塞性 CAD 定义为至少一条冠状动脉管腔狭窄≥50%。主要不良心脏事件(MACE)包括心脏死亡、非致死性心肌梗死和不稳定型心绞痛。
CMRA 上观察到 214 例(42%)阻塞性 CAD。在随访(中位时间为 5.6 年)期间,发生了 31 例 MACE。Kaplan-Meier 曲线分析显示,在 MACE(对数秩,p=0.003)和心脏死亡(p=0.012)方面,有和无阻塞性 CAD 的患者在无事件生存方面存在显著差异。无阻塞性 CAD、单支血管病变、双支血管病变、左主干或三支血管病变患者的 MACE 年化发生率分别为 0.6%、1.5%、2.3%和 3.6%(对数秩,p=0.003)。Cox 比例风险回归分析显示,在 CMRA 上的阻塞性 CAD 和临床危险因素(年龄、性别、高血压、糖尿病、血脂异常、吸烟和 CAD 家族史)中,阻塞性 CAD 和糖尿病是 MACE 的显著预测因素(风险比,2.9[p=0.005]和 2.2[p=0.034])。在多变量分析中,在调整糖尿病因素后,阻塞性 CAD 仍然是一个独立的预测因素(调整后的风险比,2.6[p=0.010])。将阻塞性 CAD 加入临床危险因素后,整体卡方值从 8.3 增加到 13.8(p=0.022)。
在长期随访中,自由呼吸式全心 CMRA 可对 MACE 和心脏死亡进行非侵入性风险分层,并为无心肌梗死或既往冠状动脉血运重建史的患者提供比传统危险因素更具增量预后价值。CMRA 检测到的阻塞性 CAD 的存在和严重程度与预后不良相关。重要的是,CMRA 上无阻塞性 CAD 的患者具有良好的预后。