Yagnik Gautam P, Seiler Jacob R, Vargas Luis A, Saxena Anshul, Narvel Raed I, Hassan Robert
Miami Orthopedics and Sports Medicine Institute, Miami, Florida, USA.
Baptist Health South Florida, Miami, Florida, USA.
Orthop J Sports Med. 2021 May 3;9(5):23259671211001773. doi: 10.1177/23259671211001773. eCollection 2021 May.
Surgical management of unstable distal clavicle fractures (DCFs) remains controversial. Traditional open techniques result in acceptable union rates but are fraught with complications. In response to these limitations, arthroscopic techniques have been developed; however, clinical outcome data are limited.
The primary purpose was to systematically evaluate the clinical and radiographic outcomes of arthroscopic fixation of unstable DCFs. The secondary purpose was to characterize the overall complication rate, focusing on major complications and subsequent reoperations.
Systematic review; Level of evidence, 4.
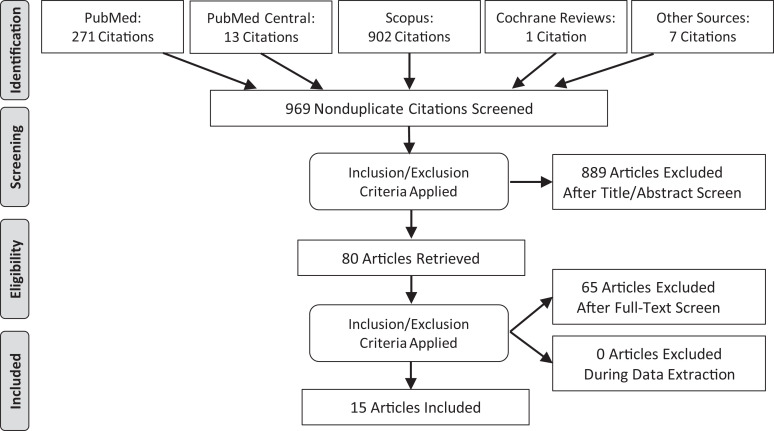
A systematic review of the literature was performed following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and included a search of the PubMed, Web of Science, Cochrane Register of Controlled Trials, EMBASE, and Scopus databases. English-language studies between 2008 and 2019 that reported on outcomes of patients with DCFs who underwent operative fixation using an arthroscopic or arthroscopically assisted surgical technique were included. Data consisted of patient characteristics, fracture type, surgical technique, concomitant injuries, union rates, functional outcomes, and complications.
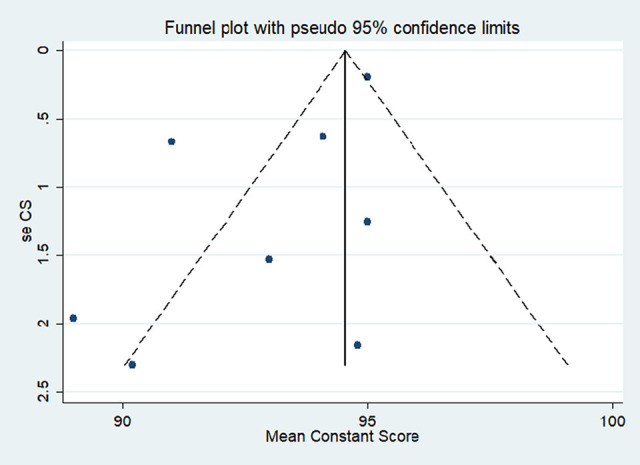
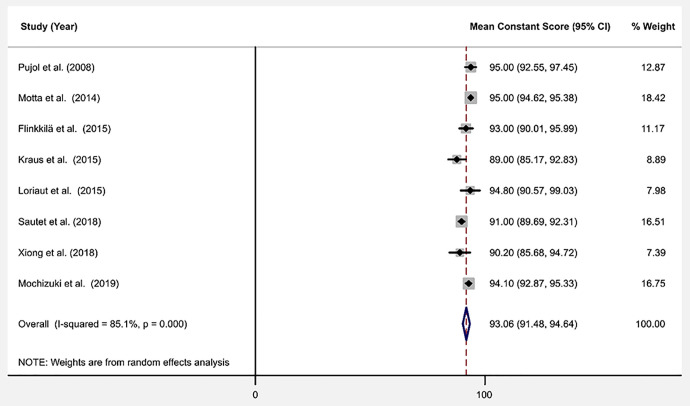
A total of 15 studies consisting of 226 DCFs treated using an arthroscopically based technique were included in the systematic review. The majority of fractures were classified as Neer type II. Most (97%) of the fractures underwent arthroscopic fixation using a cortical button coracoclavicular stabilization surgical technique. Bony union was reported in 94.1% of the fractures. Good to excellent outcomes were recorded in most patients at the final follow-up. The Constant-Murley score was the most widely used functional outcome score; the pooled mean Constant score was 93.06 (95% CI, 91.48-94.64). Complications were reported in 14 of the 15 studies, and the overall complication rate was 27.4%. However, only 12% of these were considered major complications, and only 6% required a reoperation for hardware-related complications.
Arthroscopic fixation of DCFs resulted in good functional outcomes with union rates comparable to those of traditional open techniques. While the overall complication profile was similar to that of other described techniques, there was a much lower incidence of major complications, including hardware-related complications and reoperations.
不稳定型锁骨远端骨折(DCF)的手术治疗仍存在争议。传统的开放技术能获得可接受的愈合率,但并发症频发。针对这些局限性,关节镜技术应运而生;然而,临床疗效数据有限。
主要目的是系统评估关节镜下固定不稳定型DCF的临床和影像学结果。次要目的是确定总体并发症发生率,重点关注主要并发症及后续再次手术情况。
系统评价;证据等级,4级。
按照PRISMA(系统评价和Meta分析的首选报告项目)指南对文献进行系统评价,检索了PubMed、科学网、Cochrane对照试验注册库、EMBASE和Scopus数据库。纳入2008年至2019年间的英文研究,这些研究报告了采用关节镜或关节镜辅助手术技术进行手术固定的DCF患者的结局。数据包括患者特征、骨折类型、手术技术、合并损伤、愈合率、功能结局和并发症。
系统评价共纳入15项研究,其中226例DCF采用基于关节镜的技术治疗。大多数骨折分类为Neer II型。大多数(97%)骨折采用皮质纽扣喙锁固定手术技术进行关节镜固定。94.1%的骨折实现了骨愈合。大多数患者在末次随访时获得了良好至优秀的结果。Constant-Murley评分是最广泛使用的功能结局评分;汇总后的平均Constant评分为93.06(95%CI,91.48 - 94.64)。15项研究中有14项报告了并发症,总体并发症发生率为27.4%。然而,其中仅12%被认为是主要并发症,仅6%因硬件相关并发症需要再次手术。
关节镜下固定DCF可获得良好的功能结局,愈合率与传统开放技术相当。虽然总体并发症情况与其他描述的技术相似,但主要并发症(包括硬件相关并发症和再次手术)的发生率要低得多。