Kurzawski Jacek, Janion-Sadowska Agnieszka, Zandecki Łukasz, Janion Marianna, Sadowski Marcin
Department of Cardiology, Świętokrzyskie Cardiology Centre, Kielce, Poland.
Institute of Medical Sciences, Jan Kochanowski University, Kielce, Poland.
Arch Med Sci. 2019 May 21;17(3):652-661. doi: 10.5114/aoms.2019.85249. eCollection 2021.
Ultrasound-guided thrombin injection (UGTI) is the preferred treatment of pseudoaneurysms (psA). The potential risk of complications increases with the number of UGTI treatments needed for complete psA obliteration. Identification of risk factors for recurrent psA is needed.
In total, 508 patients with femoral artery psA underwent UGTI, followed by ultrasound examination repeated twice, at 1-week intervals, to assess UGTI effectiveness. In cases of psA recurrence, the procedure was repeated. Clinical and ultrasound data were prospectively collected.
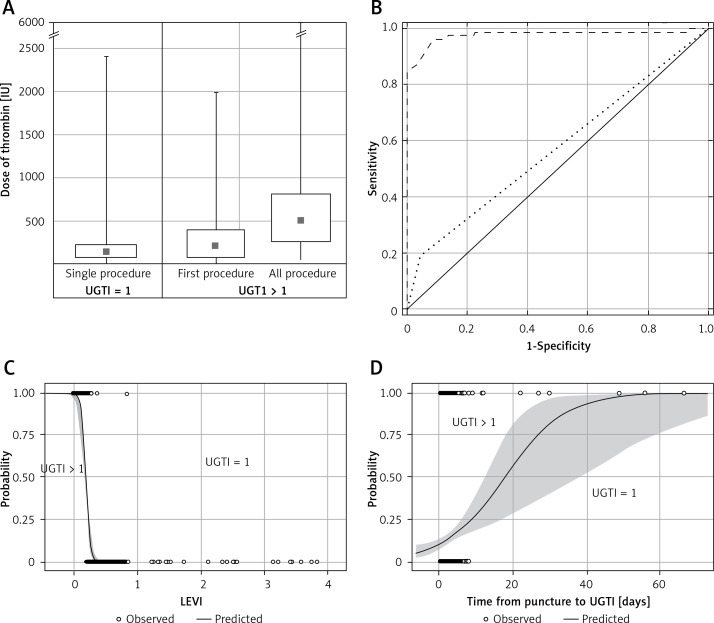
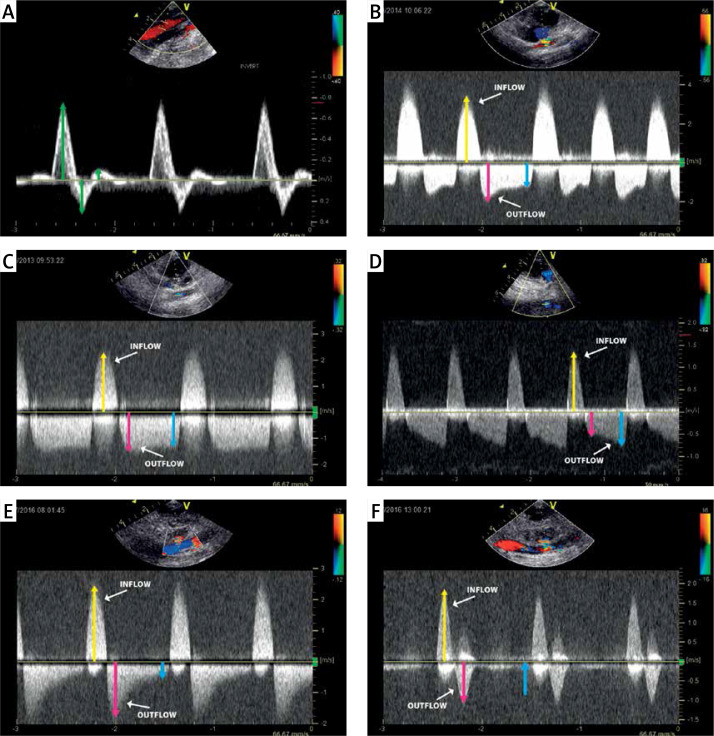
The psA recurrence occurred in 76 (15%) patients. UGTI was repeated twice in 49 (64%), three times in 15 (20%) and more than three times in 12 (16%) patients. The median thrombin dose was 150 IU (80-250 IU), and was lower in initial procedures than repeated UGTI ( = 0.025). The median psA volume was 2.26 ml (0.86-5.47 ml). The median length of the communicating channel was 4 mm (0-12 mm). A time interval between vessel catheterization and UGTI greater than 7 days ( < 0.001), a late to early velocity index (LEVI) of < 0.2 identified during the outflow phase ( < 0.001), a psA volume > 5 ml ( = 0.032), and a short communicating channel between the psA and the artery ( = 0.037) predicted psA recurrence. Antiplatelet and anticoagulant agents did not increase the risk.
The LEVI and time interval between artery cannulation and UGTI treatment are strong parameters identifying patients at risk of psA recurrence. The psA volume and communicating channel length are less substantial risks, but still significant. Concomitant antiplatelet and anticoagulant therapy do not affect the success rate of UGTI.
超声引导下凝血酶注射(UGTI)是假性动脉瘤(psA)的首选治疗方法。完全消除psA所需的UGTI治疗次数越多,并发症的潜在风险就越高。因此需要识别复发性psA的危险因素。
共有508例股动脉psA患者接受了UGTI治疗,随后每隔1周重复进行两次超声检查,以评估UGTI的有效性。对于psA复发的病例,重复该操作。前瞻性收集临床和超声数据。
76例(15%)患者出现psA复发。49例(64%)患者重复进行了两次UGTI,15例(20%)患者重复进行了三次,12例(16%)患者重复进行了三次以上。凝血酶剂量中位数为150 IU(80 - 250 IU),初次操作时的剂量低于重复UGTI时的剂量(P = 0.025)。psA体积中位数为2.26 ml(0.86 - 5.47 ml)。交通通道长度中位数为4 mm(0 - 12 mm)。血管插管与UGTI之间的时间间隔大于7天(P < 0.001)、流出期识别出的晚至早速度指数(LEVI)< 0.2(P < 0.001)、psA体积> 5 ml(P = 0.032)以及psA与动脉之间的交通通道较短(P = 0.037)可预测psA复发。抗血小板和抗凝药物不会增加风险。
LEVI以及动脉插管与UGTI治疗之间的时间间隔是识别有psA复发风险患者的重要参数。psA体积和交通通道长度是风险较小但仍具有显著意义的因素。同时使用抗血小板和抗凝治疗不影响UGTI的成功率。