Department of Nuclear Medicine, Hannover Medical School, Hannover, Germany.
Eur J Nucl Med Mol Imaging. 2021 Nov;48(12):4077-4088. doi: 10.1007/s00259-021-05412-1. Epub 2021 May 27.
Hematotoxicity is a potentially dose-limiting adverse event in patients with metastasized castration-resistant prostate cancer (mCRPC) undergoing prostate-specific membrane antigen (PSMA)-directed radioligand therapy (RLT). We aimed to identify clinical or PSMA-targeted imaging-derived parameters to predict hematological adverse events at early and late stages in the treatment course.
In 67 patients with mCRPC scheduled for Lu-PSMA-617 RLT, pretherapeutic osseous tumor volume (TV) from Ga-PSMA-11 PET/CT and laboratory values were assessed. We then tested the predictive capability of these parameters for early and late hematotoxicity (according to CTCAE vers. 5.0) after one cycle of RLT and in a subgroup of 32/67 (47.8%) patients after four cycles of RLT.
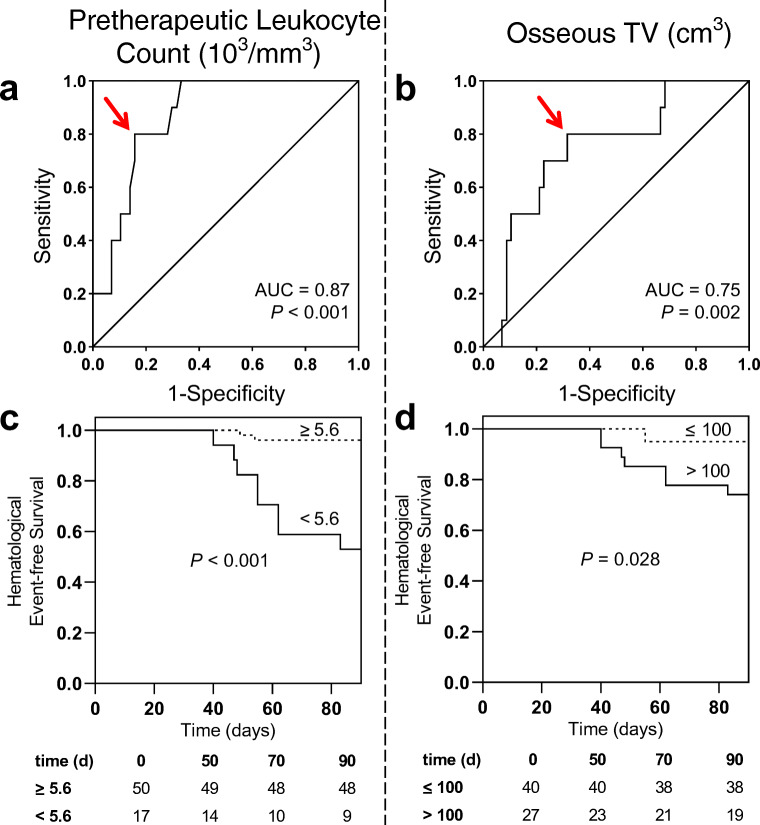
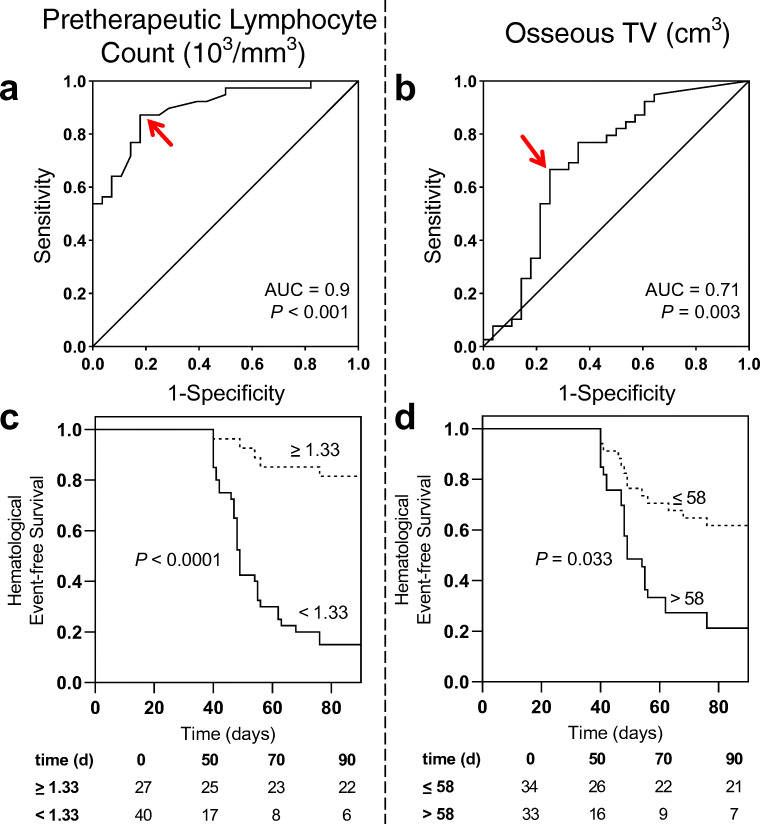
After one cycle, 10/67 (14.9%) patients developed leukocytopenia (lymphocytopenia, 39/67 [58.2%]; thrombocytopenia, 17/67 [25.4%]). A cut-off of 5.6 × 10/mm for baseline leukocytes was defined by receiver operating characteristics (ROC) and separated between patients with and without leukocytopenia (P < 0.001). Baseline leukocyte count emerged as a stronger predictive factor in multivariate analysis (hazard ratio [HR], 33.94, P = 0.001) relative to osseous TV (HR, 14.24, P = 0.01). After four cycles, 4/32 (12.5%) developed leukocytopenia and the pretherapeutic leukocyte cut-off (HR, 9.97, P = 0.082) tended to predict leukocytopenia better than TV (HR, 8.37, P = 0.109). In addition, a cut-off of 1.33 × 10/mm for baseline lymphocytes separated between patients with and without lymphocytopenia (P < 0.001), which was corroborated in multivariate analysis (HR, 21.39, P < 0.001 vs. TV, HR, 4.57, P = 0.03). After four cycles, 19/32 (59.4%) developed lymphocytopenia and the pretherapeutic cut-off for lymphocytes (HR, 46.76, P = 0.007) also demonstrated superior predictive performance for late lymphocytopenia (TV, HR, 5.15, P = 0.167). Moreover, a cut-off of 206 × 10/mm for baseline platelets separated between patients with and without thrombocytopenia (P < 0.001) and also demonstrated superior predictive capability in multivariate analysis (HR, 115.02, P < 0.001 vs.TV, HR, 12.75, P = 0.025). After four cycles, 9/32 (28.1%) developed thrombocytopenia and the pretherapeutic cut-off for platelets (HR, 5.44, P = 0.048) was also superior for the occurrence of late thrombocytopenia (TV, HR, 1.44, P = 0.7).
Pretherapeutic leukocyte, lymphocyte, and platelet levels themselves are strong predictors for early and late hematotoxicity under PSMA-directed RLT, and are better suited than PET-based osseous TV for this purpose.
在接受前列腺特异性膜抗原(PSMA)导向放射性配体治疗(RLT)的转移性去势抵抗性前列腺癌(mCRPC)患者中,血液毒性是潜在的剂量限制不良事件。我们旨在确定临床或 PSMA 靶向成像衍生参数,以预测治疗过程中早期和晚期的血液不良事件。
在 67 名计划接受 Lu-PSMA-617 RLT 的 mCRPC 患者中,评估 Ga-PSMA-11 PET/CT 的治疗前骨肿瘤体积(TV)和实验室值。然后,我们测试了这些参数在接受一个周期 RLT 后和在 32/67(47.8%)名患者的四个周期 RLT 后早期和晚期血液毒性(根据 CTCAE 版本 5.0)的预测能力。
在一个周期后,10/67(14.9%)的患者出现白细胞减少症(淋巴细胞减少症,39/67[58.2%];血小板减少症,17/67[25.4%])。通过受试者工作特征(ROC)定义了基线白细胞 5.6×10/mm 的截断值,并将其与有无白细胞减少症的患者区分开来(P<0.001)。在多变量分析中,基线白细胞计数(危险比[HR],33.94,P=0.001)比骨 TV(HR,14.24,P=0.01)更能作为强有力的预测因素。在四个周期后,4/32(12.5%)的患者出现白细胞减少症,治疗前白细胞截断值(HR,9.97,P=0.082)比 TV(HR,8.37,P=0.109)更能预测白细胞减少症。此外,基线淋巴细胞 1.33×10/mm 的截断值将有无淋巴细胞减少症的患者区分开来(P<0.001),这在多变量分析中得到了证实(HR,21.39,P<0.001 与 TV,HR,4.57,P=0.03)。在四个周期后,19/32(59.4%)的患者出现淋巴细胞减少症,治疗前淋巴细胞的截断值(HR,46.76,P=0.007)也表现出对晚期淋巴细胞减少症的良好预测性能(TV,HR,5.15,P=0.167)。此外,基线血小板 206×10/mm 的截断值将有无血小板减少症的患者区分开来(P<0.001),并且在多变量分析中也显示出更好的预测能力(HR,115.02,P<0.001 与 TV,HR,12.75,P=0.025)。在四个周期后,9/32(28.1%)的患者出现血小板减少症,治疗前血小板的截断值(HR,5.44,P=0.048)也更适合预测晚期血小板减少症(TV,HR,1.44,P=0.7)。
治疗前白细胞、淋巴细胞和血小板水平本身是 PSMA 指导 RLT 中早期和晚期血液毒性的强预测因子,并且比基于 PET 的骨 TV 更适合用于此目的。