Department of Cardiovascular Sciences and National Institute for Health Research Leicester Biomedical Research Centre, Glenfield Hospital, Groby Road, Leicester LE3 9QP, UK.
Department of Forensic Medicine, Victorian Institute of Forensic Medicine, Monash University, Melbourne, VIC, Australia.
Cardiovasc Res. 2022 Jun 22;118(7):1835-1848. doi: 10.1093/cvr/cvab183.
Spontaneous coronary artery dissection (SCAD) is a cause of acute coronary syndromes and in rare cases sudden cardiac death (SCD). Connective tissue abnormalities, coronary inflammation, increased coronary vasa vasorum (VV) density, and coronary fibromuscular dysplasia have all been implicated in the pathophysiology of SCAD but have not previously been systematically assessed. We designed a study to investigate the coronary histological and dermal collagen ultrastructural findings in SCAD.
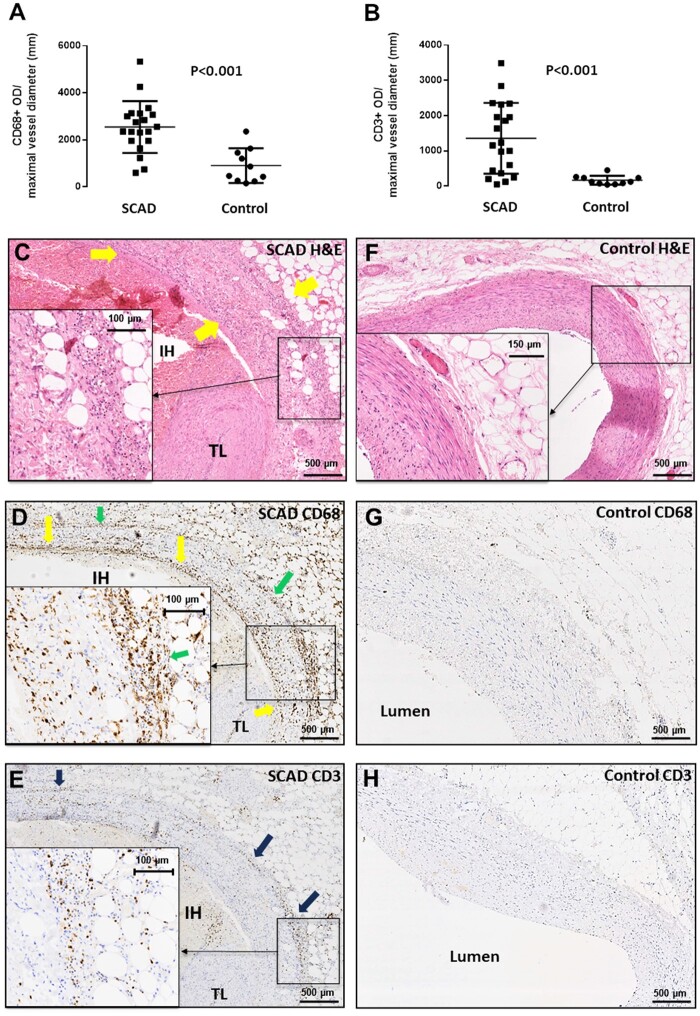
Thirty-six autopsy SCAD cases were compared with 359 SCAD survivors. Coronary and myocardial histology and immunohistochemistry were undertaken. Transmission electron microscopy (TEM) of dermal extracellular matrix (ECM) components of n = 31 SCAD survivors and n = 16 healthy volunteers were compared. Autopsy cases were more likely male (19% vs. 5%; P = 0.0004) with greater proximal left coronary involvement (56% vs. 18%; P < 0.0001) compared to SCAD survivors. N = 24 (66%) of cases showed no myocardial infarction on macro- or microscopic examination consistent with arrhythmogenic death. There was significantly (P < 0.001) higher inflammation in cases with delayed-onset death vs. sudden death and significantly more inflammation surrounding the dissected vs. non-dissected vessel segments. N = 17 (47%) cases showed limited intimal fibro-elastic thickening but no features of fibromuscular dysplasia and no endothelial or internal elastic lamina abnormalities. There were no differences in VV density between SCAD and control cases. TEM revealed no general ultrastructural differences in ECM components or markers of fibroblast metabolic activity.
Assessment of SCD requires careful exclusion of SCAD, particularly in cases without myocardial necrosis. Peri-coronary inflammation in SCAD is distinct from vasculitides and likely a reaction to, rather than a cause for SCAD. Coronary fibromuscular dysplasia or increased VV density does not appear pathophysiologically important. Dermal connective tissue changes are not common in SCAD survivors.
自发性冠状动脉夹层(SCAD)是急性冠状动脉综合征的一个原因,在极少数情况下也是心脏性猝死(SCD)的原因。结缔组织异常、冠状动脉炎症、冠状动脉血管新生(VV)密度增加以及冠状动脉纤维肌性发育不良都与 SCAD 的病理生理学有关,但以前没有进行系统评估。我们设计了一项研究,以调查 SCAD 的冠状动脉组织学和皮肤胶原超微结构发现。
将 36 例尸检 SCAD 病例与 359 例 SCAD 幸存者进行比较。进行了冠状动脉和心肌组织学及免疫组织化学检查。对 31 例 SCAD 幸存者和 16 例健康志愿者的皮肤细胞外基质(ECM)成分的透射电子显微镜(TEM)进行了比较。与 SCAD 幸存者相比,尸检病例更可能为男性(19% vs. 5%;P=0.0004),且更可能存在左冠状动脉近端受累(56% vs. 18%;P<0.0001)。在宏观或微观检查中,24 例(66%)病例未见心肌梗死,符合心律失常性死亡。与猝死相比,迟发性死亡的病例炎症明显更高(P<0.001),且炎症更常见于夹层与非夹层血管段周围。17 例(47%)病例表现为局限性内膜纤维弹性增厚,但无纤维肌性发育不良特征,且无内皮或内弹力膜异常。SCAD 病例与对照组的 VV 密度无差异。TEM 显示 ECM 成分或成纤维细胞代谢活性标志物无一般超微结构差异。
评估 SCD 需要仔细排除 SCAD,特别是在没有心肌坏死的情况下。SCAD 中的冠状动脉炎症与血管炎不同,可能是对 SCAD 的反应,而不是 SCAD 的原因。冠状动脉纤维肌性发育不良或 VV 密度增加似乎在病理生理学上并不重要。SCAD 幸存者的皮肤结缔组织改变并不常见。