Center for Reproductive Medicine, Department of Obstetrics and Gynecology, Peking University Third Hospital, Beijing, China.
National Clinical Research Center for Obstetrics and Gynecology, Key Laboratory of Assisted Reproduction, Ministry of Education, Beijing Key Laboratory of Reproductive Endocrinology and Assisted Reproductive Technology, Peking University Third Hospital, Beijing, China.
Hum Reprod. 2021 Aug 18;36(9):2452-2462. doi: 10.1093/humrep/deab155.
Is ovarian stimulation with follitropin delta in its individualised fixed-dose regimen at least as efficacious as follitropin alfa in a conventional dosing regimen in Asian population?
Ovarian stimulation with individualised follitropin delta dosing resulted in a non-inferior ongoing pregnancy rate, a significantly higher live birth rate and a significantly lower incidence of early ovarian hyperstimulation syndrome (OHSS) and/or preventive interventions compared to conventional follitropin alfa dosing.
Previous randomised controlled trials conducted in Japan as well as in Europe, North- and South America have demonstrated that ovarian stimulation with the individualised follitropin delta dosing regimen based on serum anti-Müllerian hormone (AMH) level and body weight modulated the ovarian response and reduced the risk of OHSS without compromising pregnancy and live birth rates.
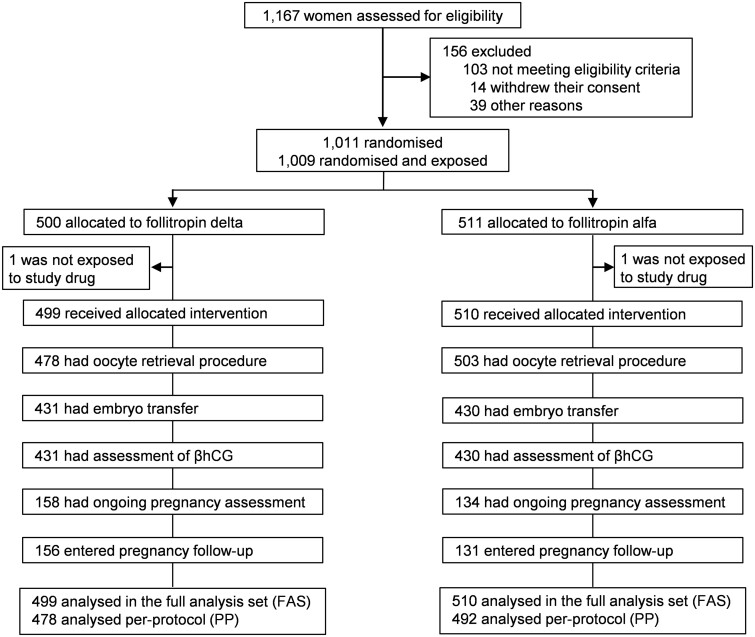
STUDY DESIGN, SIZE, DURATION: Randomised, controlled, multi-centre, assessor-blind trial conducted in 1009 Asian patients from mainland China, South Korea, Vietnam and Taiwan, undergoing their first IVF/ICSI cycle. Randomisation was stratified by age (<35, 35-37, 38-40 years). The primary endpoint was ongoing pregnancy rate assessed 10-11 weeks after embryo transfer in the fresh cycle (non-inferiority limit -10.0%; analysis adjusted for age stratum).
PARTICIPANTS/MATERIALS, SETTING, METHODS: The follitropin delta treatment consisted of a fixed daily dose individualised according to each patient's initial AMH level and body weight (AMH <15 pmol/l: 12 μg; AMH ≥15 pmol/l: 0.19 to 0.10 μg/kg; min-max 6-12 μg). The follitropin alfa dose was 150 IU/day for the first 5 days with subsequent potential dose adjustments according to individual response. A GnRH antagonist protocol was applied. OHSS was classified based on Golan's system. Women with an ongoing pregnancy were followed until live birth and 4 weeks after.
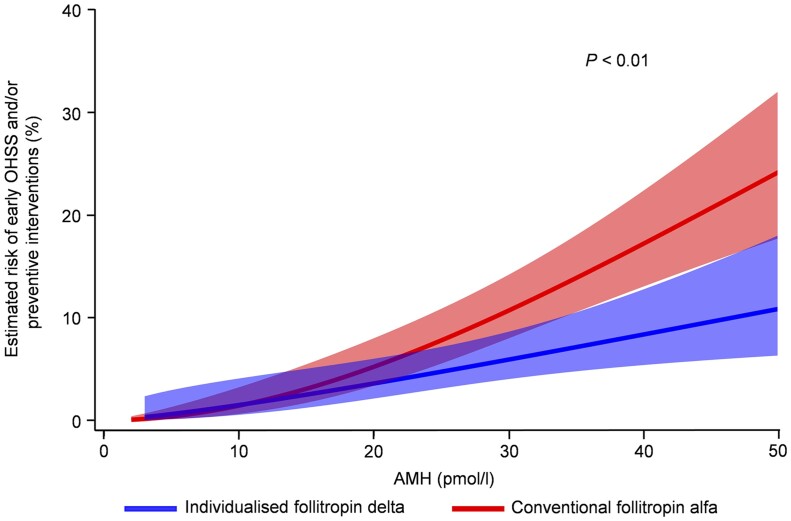
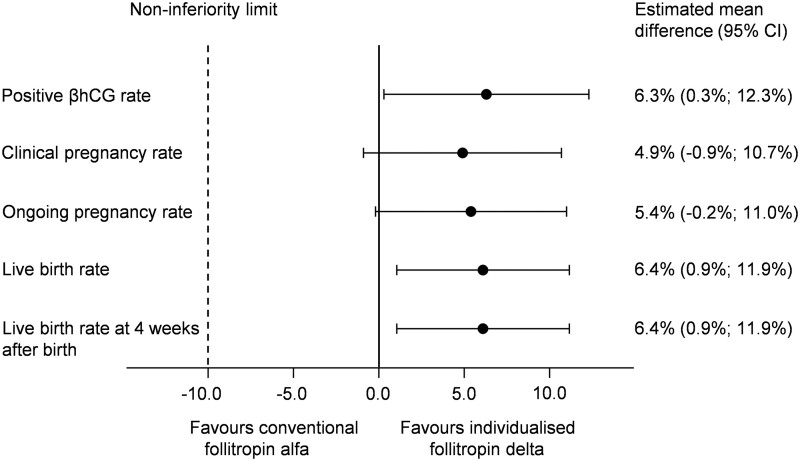
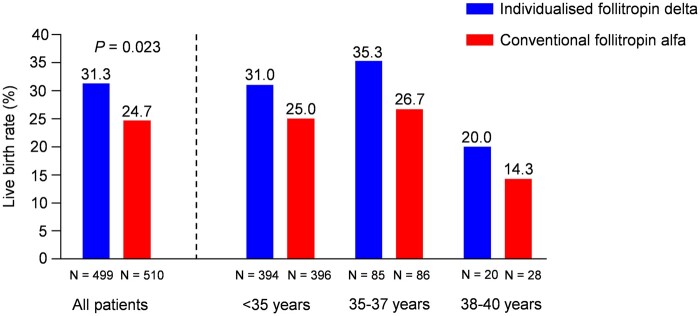
The number of oocytes retrieved was significantly (P < 0.001) lower with individualised follitropin delta versus conventional follitropin alfa (10.0 ± 6.1 versus 12.4 ± 7.3). Nevertheless, compared to the conventional dosing approach, the individualised follitropin delta dosing regimen resulted in on average 2 more oocytes (9.6 ± 5.3 versus 7.6 ± 3.5) in potential low responders as indicated by AMH <15 pmol/l, and on average 3 fewer oocytes (10.1 ± 6.3 versus 13.8 ± 7.5) in potential high responders as indicated by AMH ≥15 pmol/l. Among women with AMH ≥15 pmol/l, excessive response occurred less frequently with individualised follitropin delta than with follitropin alfa (≥15 oocytes: 20.2% versus 39.1%; ≥20 oocytes: 6.7% versus 18.5%; both P < 0.001). The incidence of early OHSS and/or preventive interventions for early OHSS was significantly (P = 0.004) reduced from 9.6% with follitropin alfa to 5.0% with individualised follitropin delta. The total gonadotropin use was significantly (P < 0.001) reduced from an average of 109.9 ± 32.9 μg (1498 ± 448 IU) follitropin alfa to 77.5 ± 24.4 μg follitropin delta. Non-inferiority of follitropin delta in its individualised dosing regimen to conventional follitropin alfa was established with respect to the primary endpoint of ongoing pregnancy rate which was 31.3% with follitropin delta compared to 25.7% with follitropin alfa (estimated mean difference 5.4% [95% CI: -0.2%; 11.0%]). The live birth rate was significantly higher at 31.3% with individualised follitropin delta compared to 24.7% with follitropin alfa (estimated mean difference 6.4% [95% CI: 0.9%; 11.9%]; P = 0.023). The live birth rate for each stratum were as follows for follitropin delta and follitropin alfa, respectively; <35 years: 31.0% versus 25.0%, 35-37 years: 35.3% versus 26.7%, 38-40 years: 20.0% versus 14.3%.
LIMITATIONS, REASONS FOR CAUTION: The trial only covered the clinical outcome of one treatment cycle with fresh cleavage-stage embryo transfers.
The present trial shows that in addition to reducing the early OHSS risk, follitropin delta in its individualised fixed-dose regimen has the potential to improve the success rate in fresh cycles across all ages and with a lower gonadotropin consumption compared to conventional follitropin alfa dosing.
STUDY FUNDING/COMPETING INTEREST(S): This study was funded by Ferring Pharmaceuticals. J.Q., Y.Z., X.L., T.H., H.-Y.H. and S.-H.K. have received institutional (not personal) clinical trial fees from Ferring Pharmaceuticals. M.G., B.M. and J.-C.A. are employees of Ferring Pharmaceuticals. J.-C.A. has pending and issued patent applications in the WO 2013/020996 and WO 2019/043143 patent families that comprise allowed and granted patent rights related to follitropin delta.
NCT03296527 (clinicaltrials.gov).
28 September 2017.
DATE OF FIRST PATIENT’S ENROLMENT: 1 December 2017.
在亚洲人群中,与传统剂量方案相比,使用固定剂量的个体化卵泡刺激素 δ 是否至少与卵泡刺激素 α 一样有效?
与传统的卵泡刺激素 α 剂量方案相比,个体化卵泡刺激素 δ 给药方案导致持续妊娠率无差异,但活产率显著提高,早期卵巢过度刺激综合征(OHSS)和/或预防干预的发生率显著降低。
以前在日本以及欧洲、北美和南美进行的随机对照试验表明,基于血清抗苗勒管激素(AMH)水平和体重的个体化卵泡刺激素 δ 给药方案调节了卵巢反应,降低了 OHSS 的风险,而不影响妊娠和活产率。
研究设计、大小、持续时间:在中国内地、韩国、越南和中国台湾的 1009 名接受首次体外受精/卵胞浆内单精子注射(IVF/ICSI)周期的亚洲患者中进行了一项随机、对照、多中心、评估者盲法试验。随机分组按年龄(<35 岁、35-37 岁、38-40 岁)分层。主要终点是新鲜周期中胚胎移植后 10-11 周的持续妊娠率(非劣效性下限-10.0%;分析调整了年龄分层)。
参与者/材料、设置、方法:卵泡刺激素 δ 治疗包括根据每位患者的初始 AMH 水平和体重个体化的固定日剂量(AMH<15 pmol/l:12μg;AMH≥15 pmol/l:0.19 至 0.10μg/kg;最小-最大 6-12μg)。卵泡刺激素 α 的剂量为 150IU/天,前 5 天,随后根据个体反应进行潜在剂量调整。应用 GnRH 拮抗剂方案。根据 Golan 系统对 OHSS 进行分类。有持续妊娠的妇女一直随访至活产和 4 周后。
与传统的卵泡刺激素 α 相比,个体化卵泡刺激素 δ 导致的获卵数显著减少(P<0.001)(10.0±6.1 与 12.4±7.3)。尽管如此,与传统的给药方法相比,个体化卵泡刺激素 δ 给药方案平均使潜在的低反应者(AMH<15 pmol/l)多获得 2 个卵母细胞(9.6±5.3 与 7.6±3.5),使潜在的高反应者(AMH≥15 pmol/l)少获得 3 个卵母细胞(10.1±6.3 与 13.8±7.5)。在 AMH≥15 pmol/l 的女性中,与卵泡刺激素 α 相比,个体化卵泡刺激素 δ 较少发生过度反应(≥15 个卵母细胞:20.2% 与 39.1%;≥20 个卵母细胞:6.7% 与 18.5%;均 P<0.001)。早期 OHSS 和/或早期 OHSS 的预防干预发生率也显著降低(P=0.004),从卵泡刺激素 α 的 9.6%降至个体化卵泡刺激素 δ 的 5.0%。总的促性腺激素使用量也显著减少(P<0.001),从平均 109.9±32.9μg(1498±448IU)卵泡刺激素 α 降至 77.5±24.4μg 卵泡刺激素 δ。个体化卵泡刺激素 δ 在其固定剂量方案中的非劣效性已在主要终点持续妊娠率方面得到证实,与卵泡刺激素 α 相比,其持续妊娠率为 31.3%,而卵泡刺激素 α 为 25.7%(估计平均差异 5.4%[-0.2%;11.0%])。与卵泡刺激素 α 相比,个体化卵泡刺激素 δ 的活产率显著更高,为 31.3%,而卵泡刺激素 α 为 24.7%(估计平均差异 6.4%[95%CI:0.9%;11.9%];P=0.023)。卵泡刺激素 δ 和卵泡刺激素 α 的每个亚组的活产率如下:<35 岁:31.0%与 25.0%,35-37 岁:35.3%与 26.7%,38-40 岁:20.0%与 14.3%。
局限性、谨慎的原因:该试验仅涵盖新鲜卵裂期胚胎移植一个治疗周期的临床结局。
本研究表明,除了降低早期 OHSS 风险外,个体化卵泡刺激素 δ 固定剂量方案还具有改善所有年龄段新鲜周期成功率的潜力,与传统的卵泡刺激素 α 剂量方案相比,还可降低促性腺激素的消耗。
研究基金/利益冲突:本研究由 Ferring 制药公司资助。J.Q.、Y.Z.、X.L.、T.H.、H.-Y.H.和 S.-H.K. 从 Ferring 制药公司获得了机构(非个人)临床试验费用。M.G.、B.M.和 J.-C.A. 是 Ferring 制药公司的员工。J.-C.A. 拥有涉及卵泡刺激素 δ 的 WO 2013/020996 和 WO 2019/043143 专利家族的已授权和已授予的专利申请,这些专利申请包含与卵泡刺激素 δ 相关的允许和授予的专利权利。
NCT03296527(clinicaltrials.gov)。
2017 年 9 月 28 日。
2017 年 12 月 1 日。