Yuan Xueyan, Lu Xinxing, Chao Yali, Beck Jennifer, Sinderby Christer, Xie Jianfeng, Yang Yi, Qiu Haibo, Liu Ling
Jiangsu Provincial Key Laboratory of Critical Care Medicine, Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University, Nanjing, 210009, Jiangsu, China.
Department of Pediatrics, University of Toronto, Toronto, Canada.
Crit Care. 2021 Jun 29;25(1):222. doi: 10.1186/s13054-021-03644-z.
Prolonged ventilatory support is associated with poor clinical outcomes. Partial support modes, especially pressure support ventilation, are frequently used in clinical practice but are associated with patient-ventilation asynchrony and deliver fixed levels of assist. Neurally adjusted ventilatory assist (NAVA), a mode of partial ventilatory assist that reduces patient-ventilator asynchrony, may be an alternative for weaning. However, the effects of NAVA on weaning outcomes in clinical practice are unclear.
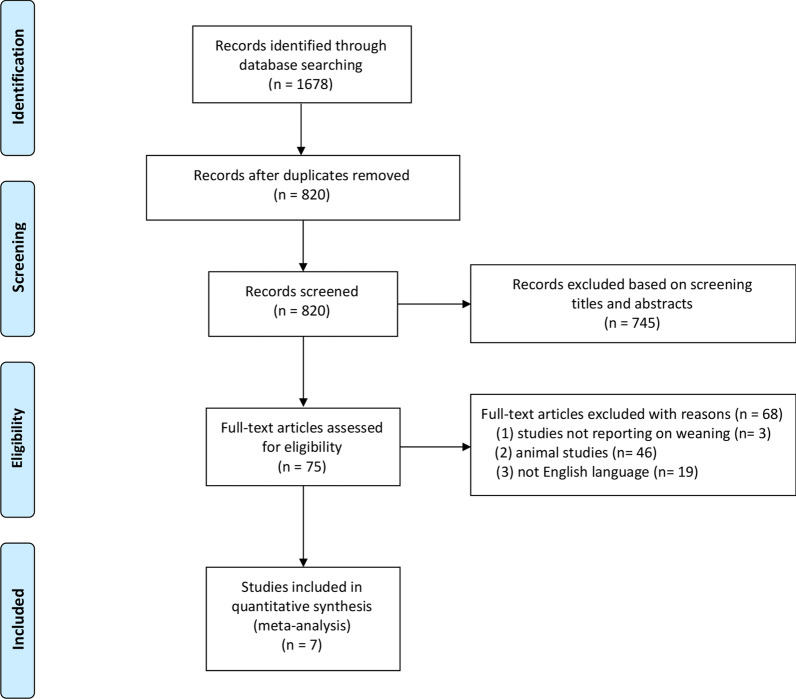
We searched PubMed, Embase, Medline, and Cochrane Library from 2007 to December 2020. Randomized controlled trials and crossover trials that compared NAVA and other modes were identified in this study. The primary outcome was weaning success which was defined as the absence of ventilatory support for more than 48 h. Summary estimates of effect using odds ratio (OR) for dichotomous outcomes and mean difference (MD) for continuous outcomes with accompanying 95% confidence interval (CI) were expressed.
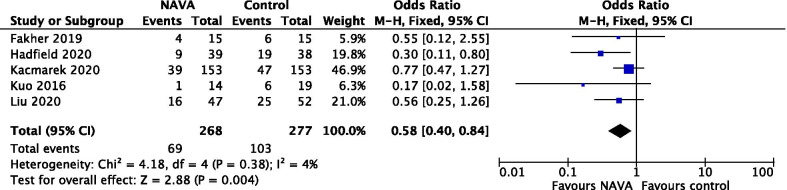
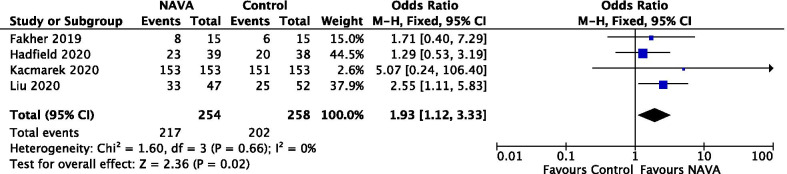
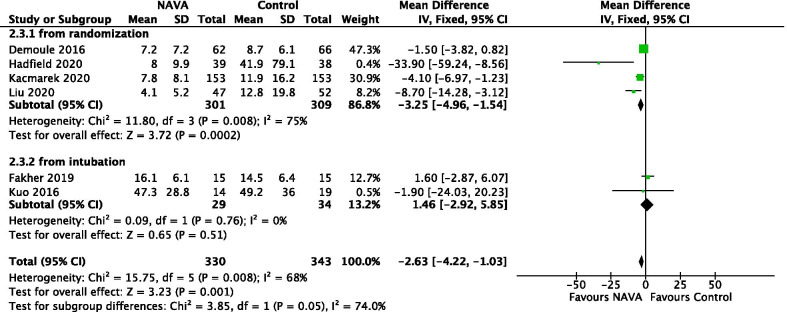
Seven studies (n = 693 patients) were included. Regarding the primary outcome, patients weaned with NAVA had a higher success rate compared with other partial support modes (OR = 1.93; 95% CI 1.12 to 3.32; P = 0.02). For the secondary outcomes, NAVA may reduce duration of mechanical ventilation (MD = - 2.63; 95% CI - 4.22 to - 1.03; P = 0.001) and hospital mortality (OR = 0.58; 95% CI 0.40 to 0.84; P = 0.004) and prolongs ventilator-free days (MD = 3.48; 95% CI 0.97 to 6.00; P = 0.007) when compared with other modes.
Our study suggests that the NAVA mode may improve the rate of weaning success compared with other partial support modes for difficult to wean patients.
长时间的通气支持与不良临床结局相关。部分支持模式,尤其是压力支持通气,在临床实践中经常使用,但与患者 - 通气不同步以及提供固定水平的辅助相关。神经调节通气辅助(NAVA)是一种可减少患者 - 呼吸机不同步的部分通气辅助模式,可能是撤机的一种替代方法。然而,NAVA在临床实践中对撤机结局的影响尚不清楚。
我们检索了2007年至2020年12月的PubMed、Embase、Medline和Cochrane图书馆。本研究纳入了比较NAVA和其他模式的随机对照试验和交叉试验。主要结局是撤机成功,定义为无通气支持超过48小时。使用二分结局的比值比(OR)和连续结局的均值差(MD)及伴随的95%置信区间(CI)表示效应的汇总估计值。
纳入了7项研究(n = 693例患者)。关于主要结局,与其他部分支持模式相比,采用NAVA撤机的患者成功率更高(OR = 1.93;95% CI 1.12至3.32;P = 0.02)。对于次要结局,与其他模式相比,NAVA可能缩短机械通气时间(MD = - 2.63;95% CI - 4.22至 - 1.03;P = 0.001)、降低医院死亡率(OR = 0.58;95% CI 0.40至0.84;P = 0.004)并延长无呼吸机天数(MD = 3.48;95% CI 0.97至6.00;P = 0.007)。
我们的研究表明,对于难以撤机的患者,与其他部分支持模式相比,NAVA模式可能提高撤机成功率。