Centre for Clinical Brain Sciences, University of Edinburgh (W.N.W.).
Nuffield Department of Population Health, University of Oxford (W.N.W.).
Stroke. 2021 Oct;52(10):3088-3096. doi: 10.1161/STROKEAHA.120.033489. Epub 2021 Jul 1.
Management of stroke risk factors might reduce later dementia. In ASCOT (Anglo-Scandinavian Outcome Trial), we determined whether dementia or stroke were associated with different blood pressure (BP)–lowering regimens; atorvastatin or placebo; and mean BP, BP variability, and mean cholesterol levels.
Participants with hypertension and ≥3 cardiovascular disease risk factors were randomly allocated to amlodipine- or atenolol-based BP-lowering regimen targeting BP <140/90 mm Hg for 5.5 years. Participants with total cholesterol ≤6.5 mmol/L were also randomly allocated to atorvastatin 10 mg or placebo for 3.3 years. Mean and LDL (low-density lipoprotein) cholesterol, BP, and SD of BP were calculated from 6 months to end of trial. UK participants were linked to electronic health records to ascertain deaths and hospitalization in general and mental health hospitals. Dementia and stroke were ascertained by validated code lists and within-trial ascertainment.
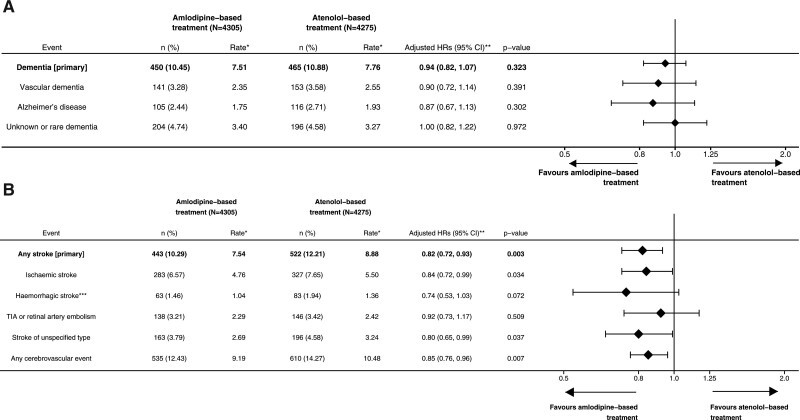
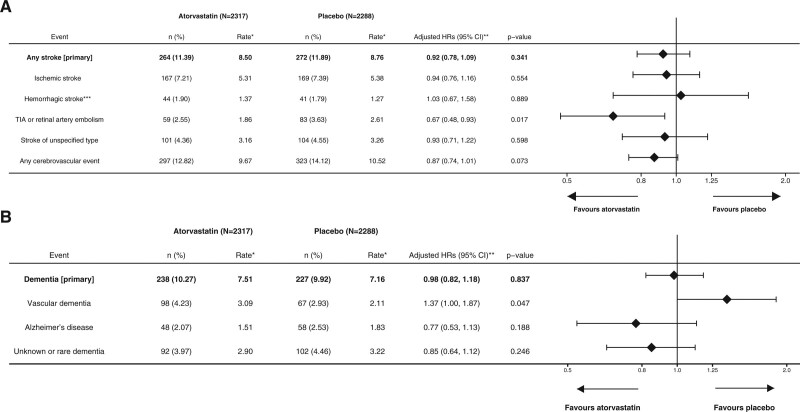
Of 8580 UK participants, 7300 were followed up to 21 years from randomization. Atorvastatin for 3.3 years had no measurable effect on stroke (264 versus 272; adjusted hazard ratio [HR], 0.92 [95% CI, 0.78–1.09]; P=0.341) or dementia (238 versus 227; adjusted HR, 0.98 [95% CI, 0.82–1.18]; P=0.837) compared with placebo. Mean total cholesterol was not associated with later stroke or dementia. An amlodipine-based compared with an atenolol-based regimen for 5.5 years reduced stroke (443 versus 522; adjusted HR, 0.82 [95% CI, 0.72–0.93]; P=0.003) but not dementia (450 versus 465; adjusted HR, 0.94 [95% CI, 0.82–1.07]; P=0.334) over follow-up. BP variability (SD mean BP) was associated with a higher risk of dementia (per 5 mm Hg HR, 1.14 [95% CI, 1.06–1.24]; P<0.001) and stroke (HR, 1.21 [95% CI, 1.12–1.32]; P<0.001) adjusted for mean BP.
An amlodipine-based BP regimen reduced the long-term incidence of stroke compared with an atenolol-based regimen but had no measurable effect on dementia. Atorvastatin had no effect on either stroke or dementia. Higher BP variability was associated with a higher incidence of later dementia and stroke.
控制中风风险因素可能会降低后期痴呆的发生风险。在 ASCOT(盎格鲁-斯堪的纳维亚心脏终点试验)中,我们确定了痴呆症或中风与不同的降压方案、阿托伐他汀或安慰剂以及平均血压、血压变异性和平均胆固醇水平之间是否存在关联。
将患有高血压且≥3 种心血管疾病风险因素的患者随机分配至氨氯地平或阿替洛尔为基础的降压方案,目标血压<140/90mmHg,持续 5.5 年。总胆固醇≤6.5mmol/L 的患者也被随机分配至阿托伐他汀 10mg 或安慰剂,持续 3.3 年。从 6 个月到试验结束,计算平均血压和 LDL(低密度脂蛋白)胆固醇、血压和血压标准差。英国参与者与电子健康记录相关联,以确定一般和精神卫生医院的死亡和住院情况。通过验证的代码列表和试验内的确定来确定痴呆症和中风的发生。
在 8580 名英国参与者中,有 7300 名参与者从随机分组到 21 年的随访中被跟踪。阿托伐他汀治疗 3.3 年对中风(264 例与 272 例;调整后的危险比 [HR],0.92[95%CI,0.78-1.09];P=0.341)或痴呆症(238 例与 227 例;调整后的 HR,0.98[95%CI,0.82-1.18];P=0.837)均无明显影响。平均总胆固醇与后期中风或痴呆症无关。与 5.5 年的阿替洛尔为基础的治疗方案相比,氨氯地平为基础的治疗方案降低了中风(443 例与 522 例;调整后的 HR,0.82[95%CI,0.72-0.93];P=0.003)但未降低痴呆症(450 例与 465 例;调整后的 HR,0.94[95%CI,0.82-1.07];P=0.334)的发生风险。血压变异性(平均血压的标准差)与痴呆症(每 5mmHg HR,1.14[95%CI,1.06-1.24];P<0.001)和中风(HR,1.21[95%CI,1.12-1.32];P<0.001)风险增加相关,这两个风险均经平均血压校正。
与阿替洛尔为基础的治疗方案相比,氨氯地平为基础的降压方案降低了长期中风的发生率,但对痴呆症没有明显影响。阿托伐他汀对中风或痴呆症均无影响。较高的血压变异性与后期痴呆症和中风的发生率增加相关。