Stock Sarah J, Horne Margaret, Bruijn Merel, White Helen, Boyd Kathleen A, Heggie Robert, Wotherspoon Lisa, Aucott Lorna, Morris Rachel K, Dorling Jon, Jackson Lesley, Chandiramani Manju, David Anna L, Khalil Asma, Shennan Andrew, van Baaren Gert-Jan, Hodgetts-Morton Victoria, Lavender Tina, Schuit Ewoud, Harper-Clarke Susan, Mol Ben W, Riley Richard D, Norman Jane E, Norrie John
Usher Institute, University of Edinburgh, Edinburgh, United Kingdom.
MRC Centre for Reproductive Health, Queen's Medical Research Institute, University of Edinburgh, United Kingdom.
PLoS Med. 2021 Jul 6;18(7):e1003686. doi: 10.1371/journal.pmed.1003686. eCollection 2021 Jul.
Timely interventions in women presenting with preterm labour can substantially improve health outcomes for preterm babies. However, establishing such a diagnosis is very challenging, as signs and symptoms of preterm labour are common and can be nonspecific. We aimed to develop and externally validate a risk prediction model using concentration of vaginal fluid fetal fibronectin (quantitative fFN), in combination with clinical risk factors, for the prediction of spontaneous preterm birth and assessed its cost-effectiveness.
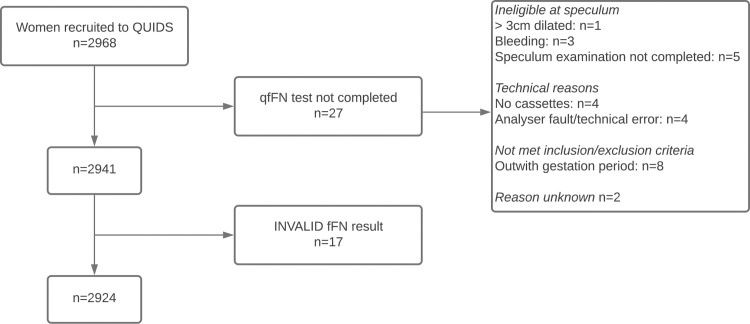
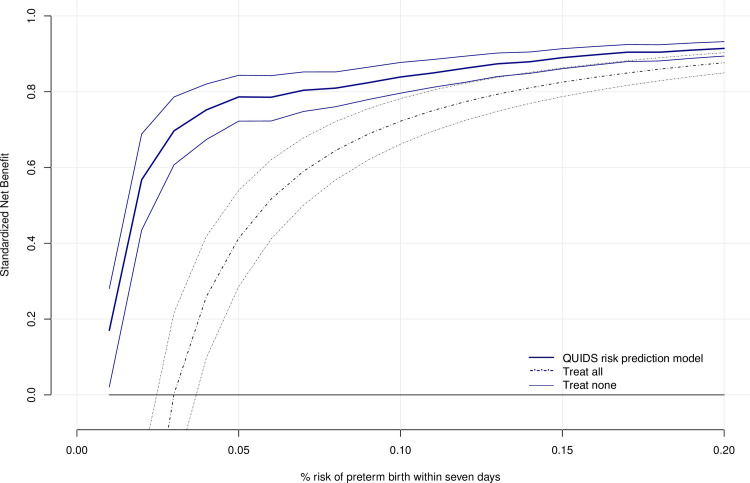
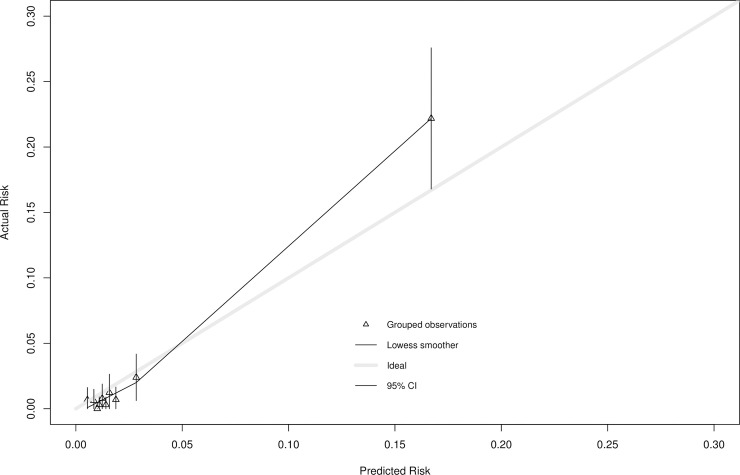
Pregnant women included in the analyses were 22+0 to 34+6 weeks gestation with signs and symptoms of preterm labour. The primary outcome was spontaneous preterm birth within 7 days of quantitative fFN test. The risk prediction model was developed and internally validated in an individual participant data (IPD) meta-analysis of 5 European prospective cohort studies (2009 to 2016; 1,783 women; mean age 29.7 years; median BMI 24.8 kg/m2; 67.6% White; 11.7% smokers; 51.8% nulliparous; 10.4% with multiple pregnancy; 139 [7.8%] with spontaneous preterm birth within 7 days). The model was then externally validated in a prospective cohort study in 26 United Kingdom centres (2016 to 2018; 2,924 women; mean age 28.2 years; median BMI 25.4 kg/m2; 88.2% White; 21% smokers; 35.2% nulliparous; 3.5% with multiple pregnancy; 85 [2.9%] with spontaneous preterm birth within 7 days). The developed risk prediction model for spontaneous preterm birth within 7 days included quantitative fFN, current smoking, not White ethnicity, nulliparity, and multiple pregnancy. After internal validation, the optimism adjusted area under the curve was 0.89 (95% CI 0.86 to 0.92), and the optimism adjusted Nagelkerke R2 was 35% (95% CI 33% to 37%). On external validation in the prospective UK cohort population, the area under the curve was 0.89 (95% CI 0.84 to 0.94), and Nagelkerke R2 of 36% (95% CI: 34% to 38%). Recalibration of the model's intercept was required to ensure overall calibration-in-the-large. A calibration curve suggested close agreement between predicted and observed risks in the range of predictions 0% to 10%, but some miscalibration (underprediction) at higher risks (slope 1.24 (95% CI 1.23 to 1.26)). Despite any miscalibration, the net benefit of the model was higher than "treat all" or "treat none" strategies for thresholds up to about 15% risk. The economic analysis found the prognostic model was cost effective, compared to using qualitative fFN, at a threshold for hospital admission and treatment of ≥2% risk of preterm birth within 7 days. Study limitations include the limited number of participants who are not White and levels of missing data for certain variables in the development dataset.
In this study, we found that a risk prediction model including vaginal fFN concentration and clinical risk factors showed promising performance in the prediction of spontaneous preterm birth within 7 days of test and has potential to inform management decisions for women with threatened preterm labour. Further evaluation of the risk prediction model in clinical practice is required to determine whether the risk prediction model improves clinical outcomes if used in practice.
The study was approved by the West of Scotland Research Ethics Committee (16/WS/0068). The study was registered with ISRCTN Registry (ISRCTN 41598423) and NIHR Portfolio (CPMS: 31277).
对出现早产迹象的女性及时进行干预,可显著改善早产婴儿的健康结局。然而,做出这样的诊断极具挑战性,因为早产的体征和症状很常见且可能不具特异性。我们旨在开发并外部验证一种风险预测模型,该模型使用阴道液中胎儿纤连蛋白的浓度(定量fFN),结合临床风险因素,来预测自发性早产,并评估其成本效益。
纳入分析的孕妇为妊娠22 + 0至34 + 6周且有早产迹象和症状者。主要结局为定量fFN检测后7天内的自发性早产。该风险预测模型在5项欧洲前瞻性队列研究(2009年至2016年;1783名女性;平均年龄29.7岁;BMI中位数24.8 kg/m²;67.6%为白人;11.7%为吸烟者;51.8%为初产妇;10.4%为多胎妊娠;139例[7.8%]在7天内发生自发性早产)的个体参与者数据(IPD)荟萃分析中开发并进行了内部验证。然后,该模型在英国26个中心的一项前瞻性队列研究(2016年至2018年;2924名女性;平均年龄28.2岁;BMI中位数25.4 kg/m²;88.2%为白人;21%为吸烟者;35.2%为初产妇;3.5%为多胎妊娠;85例[2.9%]在7天内发生自发性早产)中进行了外部验证。所开发的7天内自发性早产风险预测模型包括定量fFN、当前吸烟、非白人种族、初产和多胎妊娠。内部验证后,乐观度调整后的曲线下面积为0.89(95%CI 0.86至0.92),乐观度调整后的Nagelkerke R²为35%(95%CI 33%至37%)。在前瞻性英国队列人群中的外部验证显示,曲线下面积为0.89(95%CI 0.84至0.94),Nagelkerke R²为36%(95%CI:34%至38%)。需要对模型的截距进行重新校准以确保总体的大样本校准。校准曲线表明,在0%至10%的预测范围内,预测风险与观察到的风险之间吻合度较高,但在较高风险时存在一些校准错误(预测不足)(斜率1.24(95%CI 1.23至1.26))。尽管存在校准错误,但对于风险阈值高达约15%的情况,该模型的净效益高于“全部治疗”或“不治疗”策略。经济分析发现,与使用定性fFN相比,该预后模型在7天内早产风险≥2%作为住院和治疗阈值时具有成本效益。研究局限性包括非白人参与者数量有限以及开发数据集中某些变量的缺失数据水平。
在本研究中,我们发现一个包括阴道fFN浓度和临床风险因素的风险预测模型在预测检测后7天内自发性早产方面表现出良好的性能,并且有可能为有早产风险的女性的管理决策提供参考。需要在临床实践中对该风险预测模型进行进一步评估,以确定该风险预测模型在实际应用中是否能改善临床结局。
该研究获得了苏格兰西部研究伦理委员会的批准(16/WS/0068)。该研究已在ISRCTN注册中心(ISRCTN 41598423)和NIHR项目组合(CPMS:31277)注册。