K. Showalter, MD, Northwestern University Feinberg School of Medicine, Department of Medicine, Chicago, Illinois, and Hospital for Special Surgery, Department of Medicine, Division of Rheumatology, New York, New York.
A. Hoffmann, MS, Northwestern University Feinberg School of Medicine, Department of Medicine, Division of Rheumatology, Chicago, Illinois.
J Rheumatol. 2021 Dec;48(12):1830-1838. doi: 10.3899/jrheum.210533. Epub 2021 Jul 15.
To identify clinical factors, including esophageal dilation on chest high-resolution computed tomography (HRCT), that are associated with pulmonary function decline in patients with systemic sclerosis (SSc).
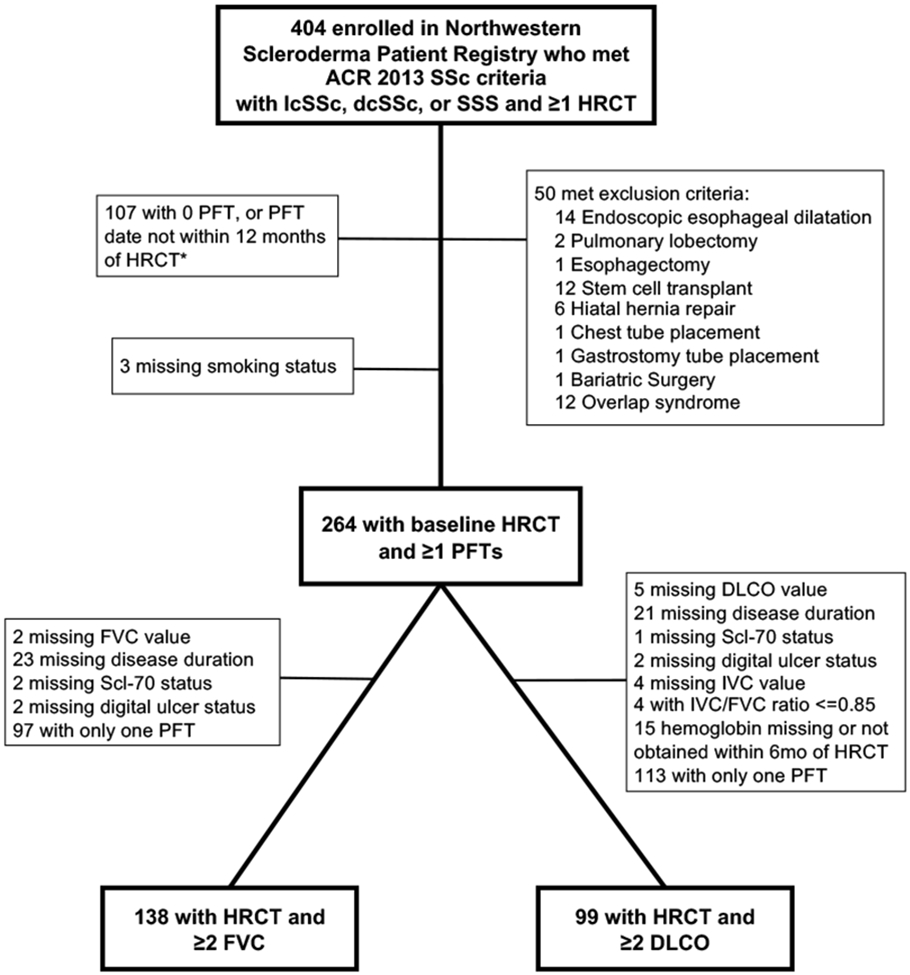
Patients fulfilled 2013 SSc criteria and had ≥ 1 HRCT and ≥ 2 pulmonary function tests (PFTs). According to published methods, widest esophageal diameter (WED) and radiographic interstitial lung disease (ILD) were assessed, and WED was dichotomized as dilated (≥ 19 mm) vs not dilated (< 19 mm). Clinically meaningful PFT decline was defined as % predicted change in forced vital capacity (FVC) ≥ 5 and/or diffusion capacity for carbon monoxide (DLCO) ≥ 15. Linear mixed effects models were used to model PFT change over time.
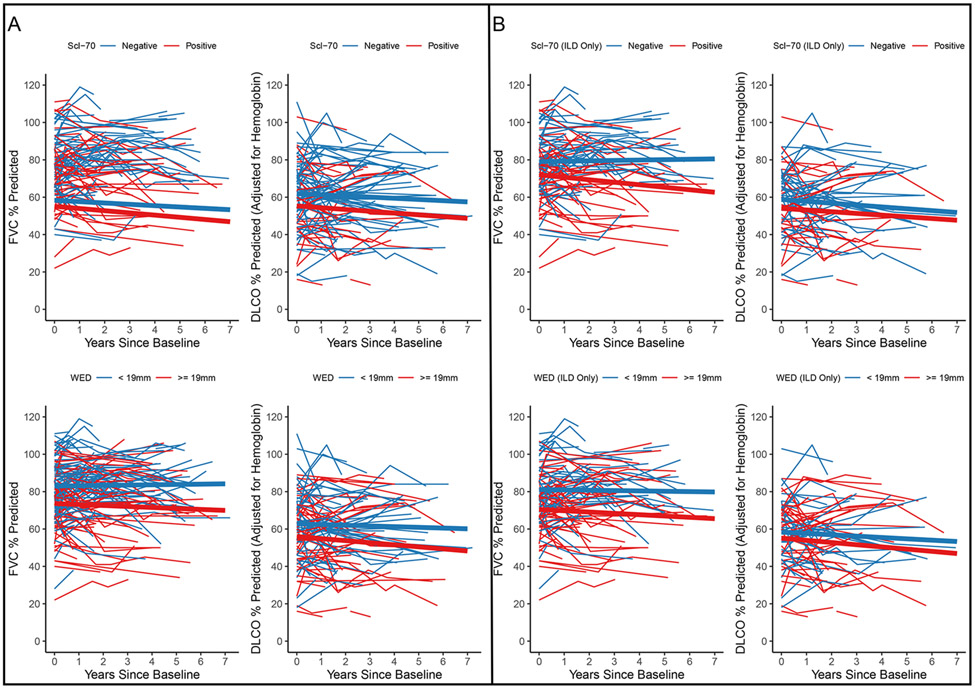
One hundred thirty-eight patients with SSc met the study criteria: 100 (72%) had radiographic ILD; 49 (35%) demonstrated FVC decline (median follow-up 2.9 yrs). Patients with antitopoisomerase I (Scl-70) autoantibodies had 5-year FVC% predicted decline (-6.33, 95% CI -9.87 to -2.79), whereas patients without Scl-70 demonstrated 5-year FVC stability (+1.78, 95% CI -0.59 to 4.15). Esophageal diameter did not distinguish between those with vs without FVC decline. Patients with esophageal dilation had statistically significant 5-year DLCO% predicted decline (-5.58, 95% CI -10.00 to -1.15), but this decline was unlikely clinically significant. Similar results were observed in the subanalysis of patients with radiographic ILD.
In patients with SSc, Scl-70 positivity is a risk factor for FVC% predicted decline at 5 years. Esophageal dilation on HRCT was associated with a minimal, nonclinically significant decline in DLCO and no change in FVC during the 5-year follow-up. These results have prognostic implications for SSc-ILD patients with esophageal dilation.
确定与系统性硬化症(SSc)患者肺功能下降相关的临床因素,包括胸部高分辨率计算机断层扫描(HRCT)上的食管扩张。
患者符合 2013 年 SSc 标准,且至少有 1 次 HRCT 和≥2 次肺功能检查(PFT)。根据已发表的方法,评估最宽食管直径(WED)和放射学间质性肺病(ILD),并将 WED 分为扩张(≥19mm)和未扩张(<19mm)。临床意义上的 PFT 下降定义为用力肺活量(FVC)预测值变化≥5%和/或一氧化碳弥散量(DLCO)≥15%。采用线性混合效应模型来模拟 PFT 随时间的变化。
共有 138 例 SSc 患者符合研究标准:100 例(72%)有放射学ILD;49 例(35%)出现 FVC 下降(中位随访 2.9 年)。抗拓扑异构酶 I(Scl-70)自身抗体阳性患者 5 年 FVC%预测值下降(-6.33,95%CI-9.87 至-2.79),而 Scl-70 阴性患者 5 年 FVC 稳定(+1.78,95%CI-0.59 至 4.15)。食管直径并不能区分 FVC 下降和未下降的患者。食管扩张的患者有统计学意义的 5 年 DLCO%预测值下降(-5.58,95%CI-10.00 至-1.15),但这种下降可能无临床意义。在放射学ILD 患者的亚分析中也观察到了类似的结果。
在 SSc 患者中,Scl-70 阳性是 5 年内 FVC%预测值下降的危险因素。HRCT 上的食管扩张与 5 年内 DLCO 的轻微、无临床意义的下降和 FVC 无变化相关。这些结果对食管扩张的 SSc-ILD 患者具有预后意义。