Committee on Genetics, Genomics and Systems Biology, The University of Chicago, Chicago, Illinois, United States of America.
Department of Medicine, and Institute of Genomics and Systems Biology, The University of Chicago, Chicago, Illinois, United States of America.
PLoS Biol. 2021 Jul 19;19(7):e3001347. doi: 10.1371/journal.pbio.3001347. eCollection 2021 Jul.
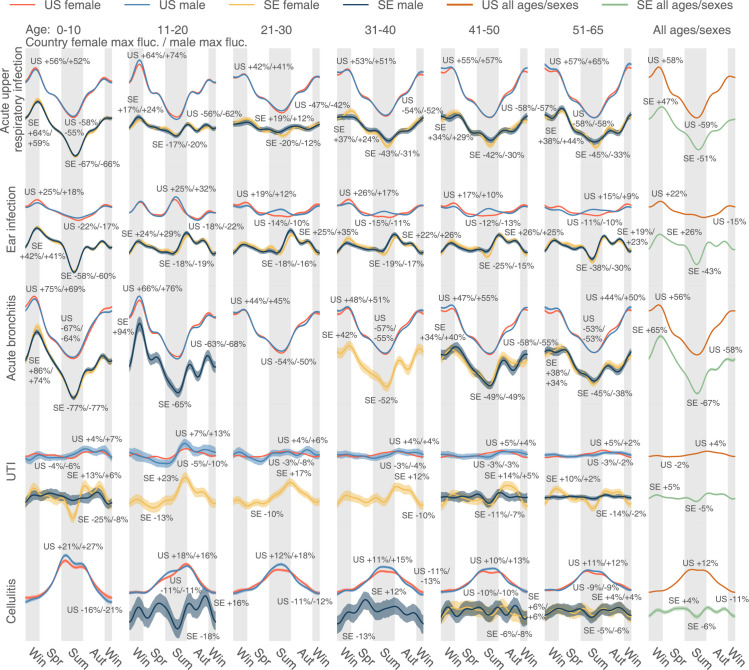
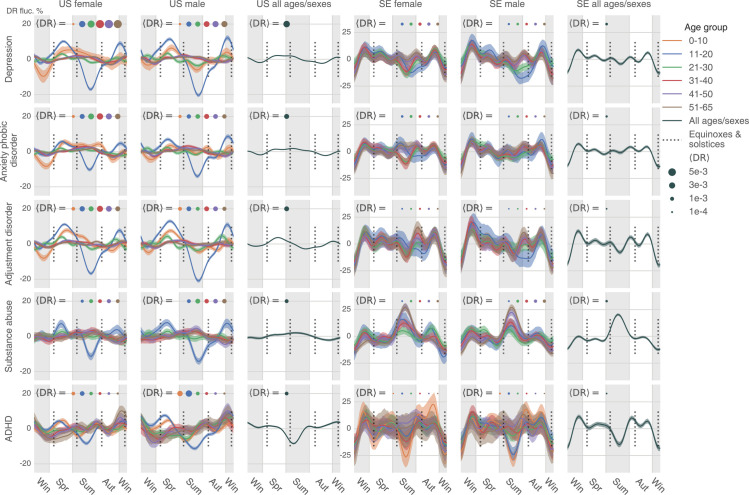
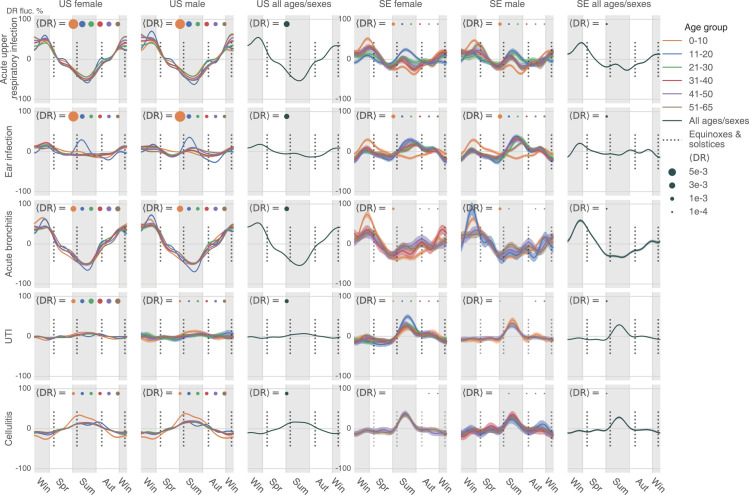
Seasonal affective disorder (SAD) famously follows annual cycles, with incidence elevation in the fall and spring. Should some version of cyclic annual pattern be expected from other psychiatric disorders? Would annual cycles be similar for distinct psychiatric conditions? This study probes these questions using 2 very large datasets describing the health histories of 150 million unique U.S. citizens and the entire Swedish population. We performed 2 types of analysis, using "uncorrected" and "corrected" observations. The former analysis focused on counts of daily patient visits associated with each disease. The latter analysis instead looked at the proportion of disease-specific visits within the total volume of visits for a time interval. In the uncorrected analysis, we found that psychiatric disorders' annual patterns were remarkably similar across the studied diseases in both countries, with the magnitude of annual variation significantly higher in Sweden than in the United States for psychiatric, but not infectious diseases. In the corrected analysis, only 1 group of patients-11 to 20 years old-reproduced all regularities we observed for psychiatric disorders in the uncorrected analysis; the annual healthcare-seeking visit patterns associated with other age-groups changed drastically. Analogous analyses over infectious diseases were less divergent over these 2 types of computation. Comparing these 2 sets of results in the context of published psychiatric disorder seasonality studies, we tend to believe that our uncorrected results are more likely to capture the real trends, while the corrected results perhaps reflect mostly artifacts determined by dominantly fluctuating, health-seeking visits across a given year. However, the divergent results are ultimately inconclusive; thus, we present both sets of results unredacted, and, in the spirit of full disclosure, leave the verdict to the reader.
季节性情感障碍(SAD)通常遵循年度周期,发病率在秋季和春季升高。其他精神障碍是否会出现类似的周期性年度模式?不同的精神疾病的年度周期是否相似?本研究使用描述 1.5 亿美国公民和整个瑞典人口健康史的两个非常大的数据集来探讨这些问题。我们进行了两种类型的分析,使用“未校正”和“校正”观察值。前者分析侧重于与每种疾病相关的每日就诊次数计数。后者分析则着眼于特定疾病就诊次数在一段时间内就诊总次数中的比例。在未校正分析中,我们发现两国研究疾病的精神障碍年度模式非常相似,瑞典的年度变化幅度明显高于美国,无论是精神疾病还是传染病。在校正分析中,只有 11 至 20 岁的患者群体再现了我们在未校正分析中观察到的所有精神障碍规律;其他年龄组与年度医疗保健就诊模式的关联发生了巨大变化。在这两种计算方法中,传染病的类似分析差异较小。在已发表的精神障碍季节性研究的背景下比较这两组结果,我们倾向于认为我们的未校正结果更有可能捕捉到真实趋势,而校正结果可能主要反映了由给定年份波动、寻求健康就诊主导的人工制品。然而,最终分歧的结果没有定论;因此,我们未删减地呈现了这两组结果,并本着充分披露的精神,将裁决留给读者。