Division of Surgical Research, Department of Surgery, University of Alberta, 3-002 Li Ka Shing Centre For Research, 11203 - 87 Ave NW, Edmonton, AB, T6G 2H5, Canada.
Division of Neurosurgery, Department of Surgery, University of Alberta, 2D Department of Surgery, University of Alberta Hospital, 8440-112 Street NW, Edmonton, AB, T6G 2B7, Canada.
BMC Neurol. 2021 Jul 24;21(1):290. doi: 10.1186/s12883-021-02323-4.
Medically-refractory trigeminal neuralgia (TN) can be treated successfully with operative intervention, but a significant proportion of patients are non-responders despite undergoing technically successful surgery. The thalamus is a key component of the trigeminal sensory pathway involved in transmitting facial pain, but the role of the thalamus in TN, and its influence on durability of pain relief after TN surgery, are relatively understudied. We aimed to test the hypothesis that variations in thalamic structure and metabolism are related to surgical non-response in TN.
We performed a longitudinal, peri-operative neuroimaging study of the thalamus in medically-refractory TN patients undergoing microvascular decompression or percutaneous balloon compression rhizotomy. Patients underwent structural MRI and MR spectroscopy scans pre-operatively and at 1-week following surgery, and were classified as responders or non-responders based on 1-year post-operative pain outcome. Thalamus volume, shape, and metabolite concentration (choline/creatine [Cho/Cr] and N-acetylaspartate/creatine [NAA/Cr]) were evaluated at baseline and 1-week, and compared between responders, non-responders, and healthy controls.
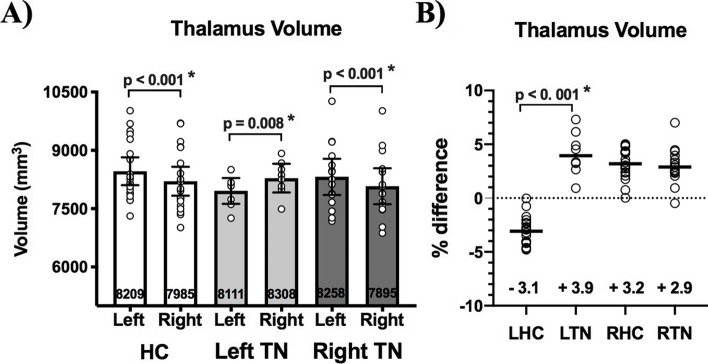
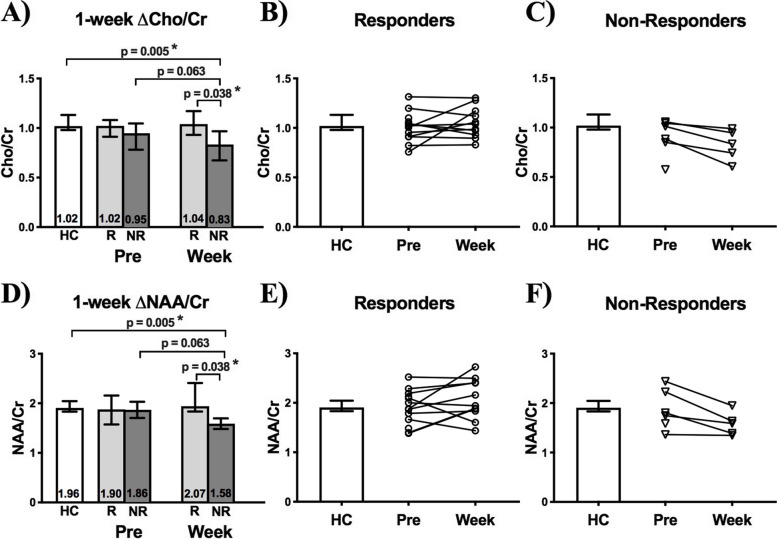
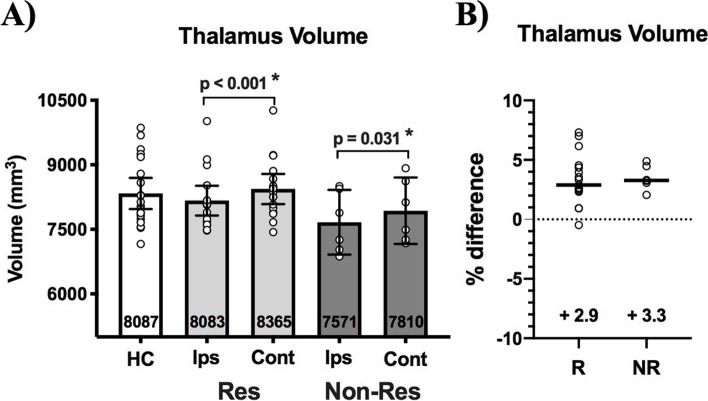
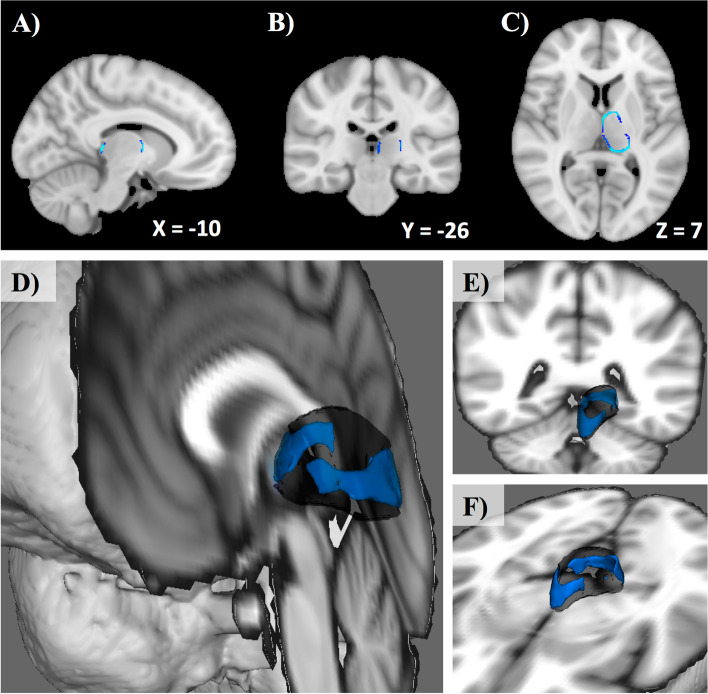
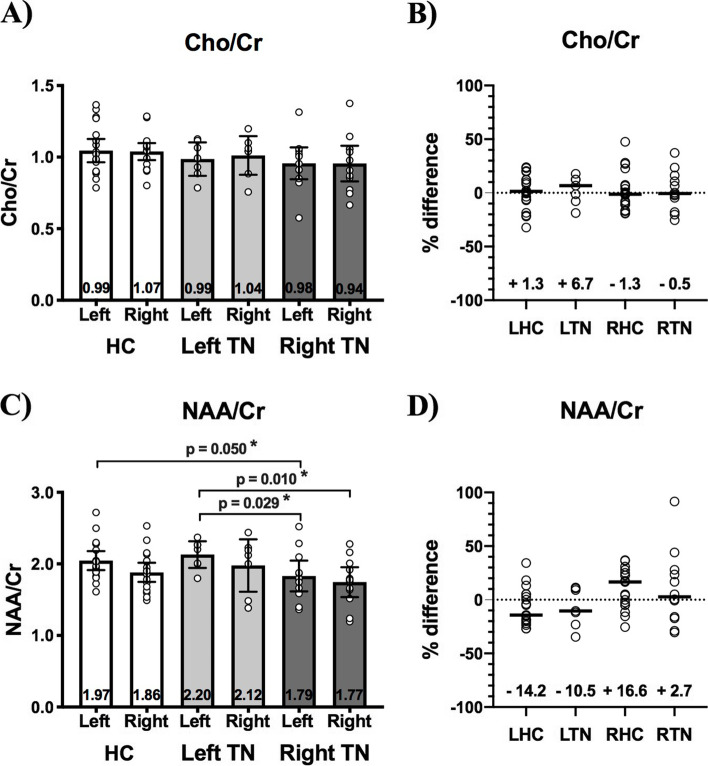
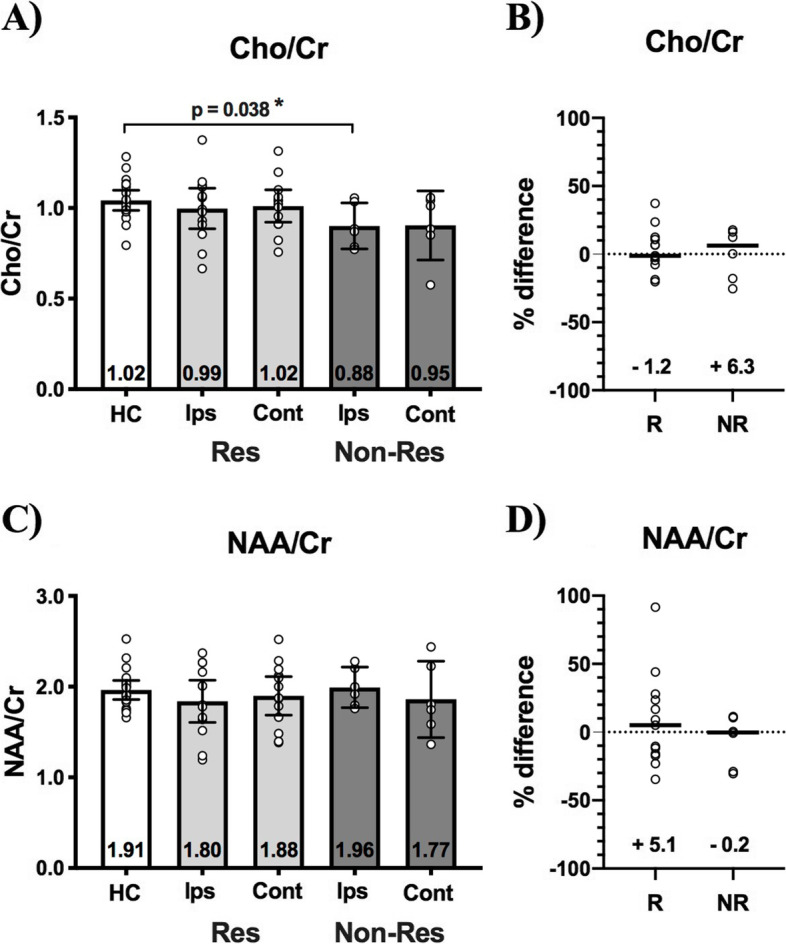
Twenty healthy controls and 23 patients with medically-refractory TN treated surgically (17 responders, 6 non-responders) were included. Pre-operatively, TN patients as a group showed significantly larger thalamus volume contralateral to the side of facial pain. However, vertex-wise shape analysis showed significant contralateral thalamus volume reduction in non-responders compared to responders in an axially-oriented band spanning the outer thalamic circumference (peak p = 0.019). Further, while pre-operative thalamic metabolite concentrations did not differ between responders and non-responders, as early as 1-week after surgery, long-term non-responders showed a distinct decrease in contralateral thalamic Cho/Cr and NAA/Cr, irrespective of surgery type, which was not observed in responders.
Atrophy of the contralateral thalamus is a consistent feature across patients with medically-refractory TN. Regional alterations in preoperative thalamic structure, and very early post-operative metabolic changes in the thalamus, both appear to influence the durability of pain relief after TN surgery.
药物难治性三叉神经痛(TN)可以通过手术干预成功治疗,但尽管手术技术成功,仍有相当一部分患者没有反应。丘脑是参与传递面部疼痛的三叉神经感觉通路的关键组成部分,但丘脑在 TN 中的作用及其对 TN 手术后疼痛缓解的持久性的影响相对研究较少。我们旨在检验这样一个假设,即丘脑结构和代谢的变化与 TN 的手术无反应有关。
我们对接受微血管减压或经皮球囊压迫脊神经根切断术的药物难治性 TN 患者进行了丘脑的纵向、围手术期神经影像学研究。患者在术前和术后 1 周进行结构 MRI 和磁共振波谱扫描,并根据术后 1 年的疼痛结果将其分类为反应者或无反应者。在基线和术后 1 周评估丘脑体积、形状和代谢物浓度(胆碱/肌酸 [Cho/Cr] 和 N-乙酰天门冬氨酸/肌酸 [NAA/Cr]),并在反应者、无反应者和健康对照组之间进行比较。
共纳入 20 名健康对照者和 23 名接受手术治疗的药物难治性 TN 患者(17 名反应者,6 名无反应者)。术前,TN 患者组表现为患侧面部疼痛对侧丘脑体积明显增大。然而,顶点-wise 形状分析显示,无反应者的丘脑体积与反应者相比在轴向方向上呈环形分布,呈明显缩小(峰值 p=0.019)。进一步,虽然反应者和无反应者之间的术前丘脑代谢物浓度没有差异,但早在术后 1 周,长期无反应者的丘脑 Cho/Cr 和 NAA/Cr 就出现了明显下降,无论手术类型如何,这在反应者中都没有观察到。
药物难治性 TN 患者的对侧丘脑萎缩是一个一致的特征。术前丘脑结构的区域性改变以及丘脑的早期术后代谢变化似乎都影响了 TN 手术后疼痛缓解的持久性。