Division of Hematology/Oncology, Department of Pediatrics, University of Toronto Developmental and Stem Cell Biology, The Hospital for Sick Children Research Institute, Toronto, Ontario, Canada.
Children's Oncology Group, University of Southern California, Monrovia, CA.
Blood. 2021 Dec 9;138(23):2337-2346. doi: 10.1182/blood.2021012206.
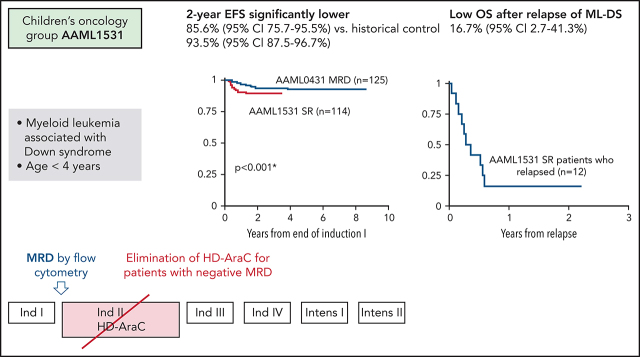
Myeloid leukemia in children with Down syndrome (ML-DS) is associated with young age and somatic GATA1 mutations. Because of high event-free survival (EFS) and hypersensitivity of the leukemic blasts to chemotherapy, the prior Children's Oncology Group protocol ML-DS protocol (AAML0431) reduced overall treatment intensity but lacking risk stratification, retained the high-dose cytarabine course (HD-AraC), which was highly associated with infectious morbidity. Despite high EFS of ML-DS, survival for those who relapse is rare. AAML1531 introduced therapeutic risk stratification based on the previously identified prognostic factor, measurable residual disease (MRD) at the end of the first induction course. Standard risk (SR) patients were identified by negative MRD using flow cytometry (<0.05%) and did not receive the historically administered HD-AraC course. Interim analysis of 114 SR patients revealed a 2-year EFS of 85.6% (95% confidence interval [CI], 75.7-95.5), which was significantly lower than for MRD- patients treated with HD-AraC on AAML0431 (P = .0002). Overall survival at 2 years was 91.0% (95% CI, 83.8-95.0). Twelve SR patients relapsed, mostly within 1 year from study entry and had a 1-year OS of 16.7% (95% CI, 2.7-41.3). Complex karyotypes were more frequent in SR patients who relapsed compared with those who did not (36% vs 9%; P = .0248). MRD by error-corrected sequencing of GATA1 mutations was piloted in 18 SR patients and detectable in 60% who relapsed vs 23% who did not (P = .2682). Patients with SR ML-DS had worse outcomes without HD-AraC after risk classification based on flow cytometric MRD.
唐氏综合征相关儿童髓系白血病(ML-DS)与年龄较小和体细胞 GATA1 突变有关。由于无事件生存(EFS)率高,且白血病细胞对化疗敏感,因此之前的儿童肿瘤学组方案 ML-DS 方案(AAML0431)降低了整体治疗强度,但缺乏风险分层,保留了高剂量阿糖胞苷疗程(HD-AraC),这与感染发病率高度相关。尽管 ML-DS 的 EFS 率很高,但复发患者的存活率却很低。AAML1531 根据之前确定的预后因素,即第一个诱导疗程结束时的可测量残留疾病(MRD),引入了治疗风险分层。通过流式细胞术(<0.05%)检测到 MRD 阴性的标准风险(SR)患者无需接受历史上给予的 HD-AraC 疗程。114 例 SR 患者的中期分析显示,2 年 EFS 为 85.6%(95%置信区间[CI],75.7-95.5),显著低于接受 AAML0431 上 HD-AraC 治疗的 MRD-患者(P=0.0002)。2 年总生存率为 91.0%(95%CI,83.8-95.0)。12 例 SR 患者复发,大多数在研究入组后 1 年内复发,1 年 OS 为 16.7%(95%CI,2.7-41.3)。与未复发的患者相比,复发的 SR 患者中复杂核型更为常见(36%比 9%;P=0.0248)。在 18 例 SR 患者中进行了 GATA1 突变的纠错测序 MRD 检测,其中 60%的复发患者可检测到 MRD,而未复发患者为 23%(P=0.2682)。在基于流式细胞术 MRD 进行风险分类后,无 HD-AraC 的 SR ML-DS 患者预后较差。