From the Infection Prevention and Control Unit (M.B., T.G., C.C., E.G.L., C.R., I.T., M.Z., G.R.-Y.), the Department of Clinical Microbiology (S.A.), General Management (Y.K.), and the Central Virology Laboratory, Public Health Authority, Ministry of Health (Y.L., M.M., V.I., N.Z.), Sheba Medical Center Tel Hashomer, Ramat Gan, Sackler School of Medicine, Tel Aviv University, Tel Aviv (T.G., Y.L., M.M., E.G.L., Y.K., G.R.-Y.), and the Laboratory Wing, Asaf Harofe Medical Center, Be'er Ya'akov (A.B.-C.) - all in Israel; St. George's School of Medicine of London and Faculty of Medicine, University of Nicosia, Nicosia, Cyprus (M.B.); and Harvard T.H. Chan School of Public Health, Boston (M.L.).
N Engl J Med. 2021 Oct 14;385(16):1474-1484. doi: 10.1056/NEJMoa2109072. Epub 2021 Jul 28.
Despite the high efficacy of the BNT162b2 messenger RNA vaccine against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), rare breakthrough infections have been reported, including infections among health care workers. Data are needed to characterize these infections and define correlates of breakthrough and infectivity.
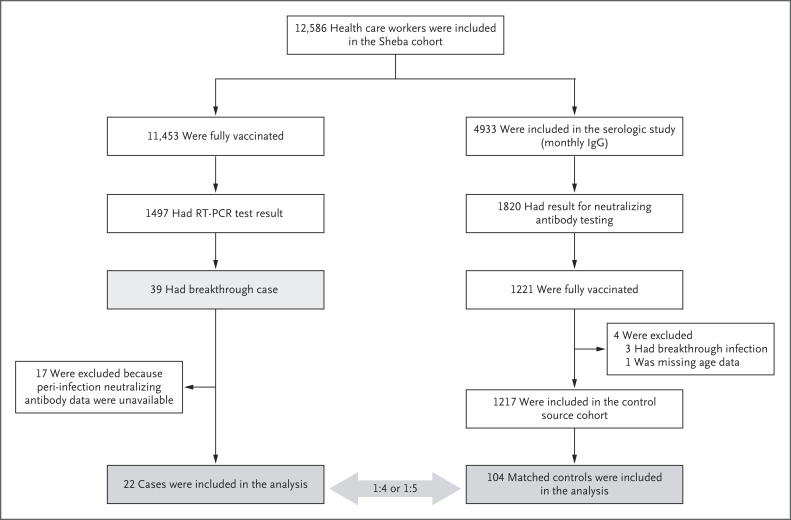
At the largest medical center in Israel, we identified breakthrough infections by performing extensive evaluations of health care workers who were symptomatic (including mild symptoms) or had known infection exposure. These evaluations included epidemiologic investigations, repeat reverse-transcriptase-polymerase-chain-reaction (RT-PCR) assays, antigen-detecting rapid diagnostic testing (Ag-RDT), serologic assays, and genomic sequencing. Correlates of breakthrough infection were assessed in a case-control analysis. We matched patients with breakthrough infection who had antibody titers obtained within a week before SARS-CoV-2 detection (peri-infection period) with four to five uninfected controls and used generalized estimating equations to predict the geometric mean titers among cases and controls and the ratio between the titers in the two groups. We also assessed the correlation between neutralizing antibody titers and N gene cycle threshold (Ct) values with respect to infectivity.
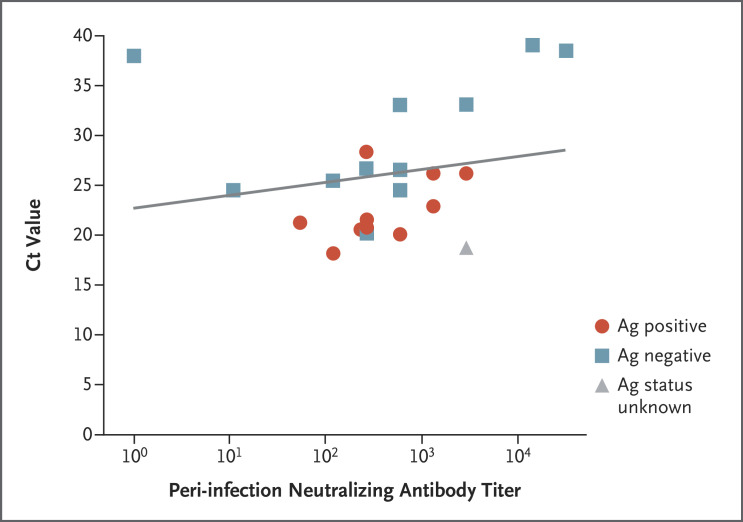
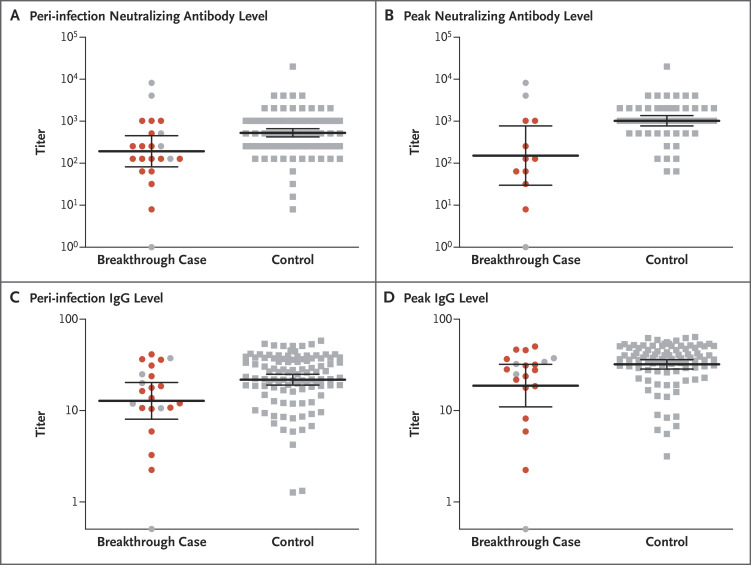
Among 1497 fully vaccinated health care workers for whom RT-PCR data were available, 39 SARS-CoV-2 breakthrough infections were documented. Neutralizing antibody titers in case patients during the peri-infection period were lower than those in matched uninfected controls (case-to-control ratio, 0.361; 95% confidence interval, 0.165 to 0.787). Higher peri-infection neutralizing antibody titers were associated with lower infectivity (higher Ct values). Most breakthrough cases were mild or asymptomatic, although 19% had persistent symptoms (>6 weeks). The B.1.1.7 (alpha) variant was found in 85% of samples tested. A total of 74% of case patients had a high viral load (Ct value, <30) at some point during their infection; however, of these patients, only 17 (59%) had a positive result on concurrent Ag-RDT. No secondary infections were documented.
Among fully vaccinated health care workers, the occurrence of breakthrough infections with SARS-CoV-2 was correlated with neutralizing antibody titers during the peri-infection period. Most breakthrough infections were mild or asymptomatic, although persistent symptoms did occur.
尽管 BNT162b2 信使 RNA 疫苗对严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)具有很高的功效,但仍有罕见的突破性感染报告,包括在医护人员中发生的感染。需要数据来描述这些感染,并确定突破性感染和传染性的相关因素。
在以色列最大的医疗中心,我们通过对有症状(包括轻度症状)或已知感染暴露的医护人员进行广泛评估,确定了突破性感染。这些评估包括流行病学调查、重复逆转录-聚合酶链反应(RT-PCR)检测、抗原检测快速诊断检测(Ag-RDT)、血清学检测和基因组测序。在病例对照分析中评估了突破性感染的相关因素。我们将在 SARS-CoV-2 检测前一周内(感染前期间)获得抗体滴度的突破性感染患者与四到五名未感染的对照进行匹配,并使用广义估计方程来预测病例和对照组的几何平均滴度以及两组之间的滴度比值。我们还评估了中和抗体滴度与 N 基因循环阈值(Ct)值与传染性的相关性。
在 1497 名完全接种疫苗的医护人员中,有 39 名发生了 SARS-CoV-2 突破性感染。在感染前期间,病例患者的中和抗体滴度低于匹配的未感染对照组(病例与对照组比值,0.361;95%置信区间,0.165 至 0.787)。较高的感染前中和抗体滴度与较低的传染性(较高的 Ct 值)相关。大多数突破性病例为轻度或无症状,尽管 19%的患者持续出现症状(>6 周)。在检测的样本中,发现 85%为 B.1.1.7(alpha)变异株。共有 74%的病例患者在感染过程中的某个时间点病毒载量较高(Ct 值<30);然而,在这些患者中,只有 17 名(59%)同时进行的 Ag-RDT 检测呈阳性。未记录到二次感染。
在完全接种疫苗的医护人员中,SARS-CoV-2 的突破性感染与感染前期间的中和抗体滴度相关。大多数突破性感染为轻度或无症状,但确实存在持续症状。