Division of Hepatology, Department of Medicine, UCLA Medical Center, David Geffen School of Medicine at UCLA, Los Angeles, California, USA.
Division of Liver and Pancreas Transplantation, Department of Surgery, UCLA Medical Center, David Geffen School of Medicine at UCLA, Los Angeles, Los Angeles, California, USA.
Clin Transl Gastroenterol. 2021 Aug 1;12(8):e00378. doi: 10.14309/ctg.0000000000000378.
The outcomes of transjugular intrahepatic portosystemic shunt (TIPS) placement in patients with hepatic encephalopathy (HE) are controversial. We studied the relationship of pre-TIPS HE in patients undergoing TIPS for refractory ascites on all-cause mortality and development of post-TIPS HE.
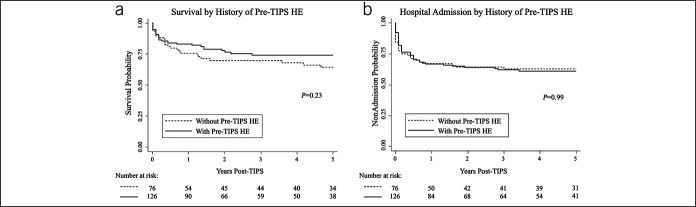
A single-center retrospective comparison study was performed for patients undergoing TIPS for refractory ascites. Survival by history of pre-TIPS HE was demonstrated with Kaplan-Meier curves. Univariate and multivariate logistic regression analyses were performed to identify the predictors of post-TIPS clinical outcomes for patients with and without pre-TIPS HE.
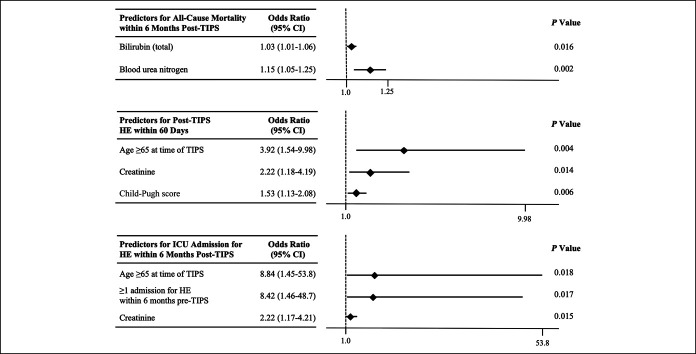
We identified 202 TIPS recipients (61% male, mean ± SD; age 59.1 ± 10.2 years; mean model for end-stage liver disease score 17.3 ± 6.9). Pre-TIPS HE did not predispose patients for increased all-cause mortality, increased risk of experiencing HE within 60 days, or increased risk of hospital admission for HE within 6 months. A multivariate analysis demonstrated that total bilirubin (odds ratio [OR] 1.03; P = 0.016) and blood urea nitrogen (OR 1.15; P = 0.002) were predictors for all-cause mortality within 6 months post-TIPS. Age ≥65 years (OR 3.92; P = 0.004), creatinine (OR 2.22; P = 0.014), and Child-Pugh score (OR 1.53; P = 0.006) were predictors for HE within 60 days post-TIPS. Predictors of intensive care admission for HE within 6 months post-TIPS included age ≥65 years (OR 8.84; P = 0.018), history of any admission for HE within 6 months pre-TIPS (OR 8.42; P = 0.017), and creatinine (OR 2.22; P = 0.015).
If controlled, pre-TIPS HE does not adversely impact patient survival or clinical outcomes, such as development of HE within 60 days of TIPS or hospital admission for HE within 6 months. Patients may be able to undergo TIPS for refractory ascites despite a history of HE.
经颈静脉肝内门体分流术(TIPS)治疗肝性脑病(HE)患者的结局存在争议。我们研究了 TIPS 治疗难治性腹水患者的术前 HE 与全因死亡率和 TIPS 后 HE 发展的关系。
对 TIPS 治疗难治性腹水的患者进行了单中心回顾性比较研究。通过 Kaplan-Meier 曲线展示了术前 HE 病史对生存率的影响。对有和无术前 HE 的患者进行单变量和多变量逻辑回归分析,以确定 TIPS 后临床结局的预测因素。
我们共纳入 202 例接受 TIPS 治疗的患者(61%为男性,平均年龄±标准差为 59.1±10.2 岁;平均终末期肝病模型评分 17.3±6.9)。术前 HE 并不会增加全因死亡率、TIPS 后 60 天内发生 HE 的风险或 TIPS 后 6 个月内因 HE 住院的风险。多变量分析表明,总胆红素(比值比 [OR] 1.03;P=0.016)和血尿素氮(OR 1.15;P=0.002)是 TIPS 后 6 个月内全因死亡的预测因素。年龄≥65 岁(OR 3.92;P=0.004)、肌酐(OR 2.22;P=0.014)和 Child-Pugh 评分(OR 1.53;P=0.006)是 TIPS 后 60 天内发生 HE 的预测因素。TIPS 后 6 个月内因 HE 入住重症监护病房的预测因素包括年龄≥65 岁(OR 8.84;P=0.018)、TIPS 前 6 个月内因 HE 住院的任何病史(OR 8.42;P=0.017)和肌酐(OR 2.22;P=0.015)。
如果得到控制,术前 HE 并不会对患者的生存或临床结局产生不利影响,如 TIPS 后 60 天内发生 HE 或 TIPS 后 6 个月内因 HE 住院。尽管有 HE 病史,患者仍可能接受 TIPS 治疗难治性腹水。