Department of Thoracic Surgery, Tel Aviv Medical Center, Affiliated with Sackler School of Medicine, Tel-Aviv University, Tel Aviv, Israel.
Department of Oncology, Shamir Medical Center, Zerifin, Affiliated with Sackler School of Medicine, Tel-Aviv University, Tel Aviv, Israel.
Sci Rep. 2021 Oct 12;11(1):20232. doi: 10.1038/s41598-021-99271-3.
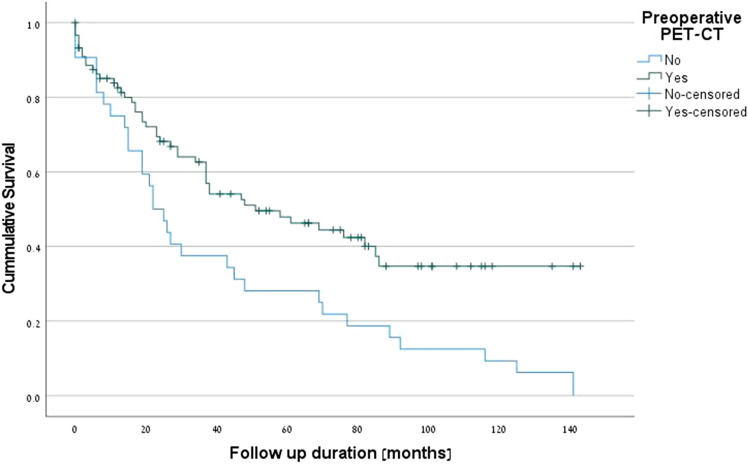
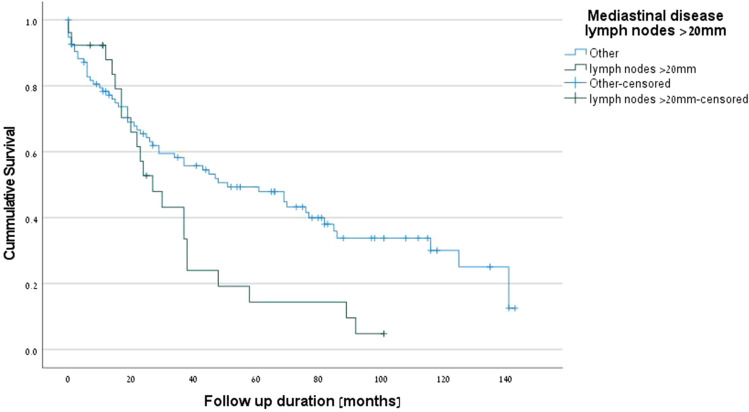
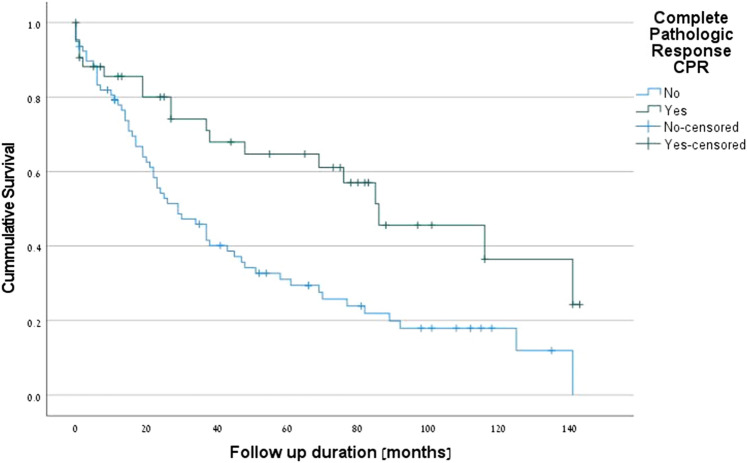
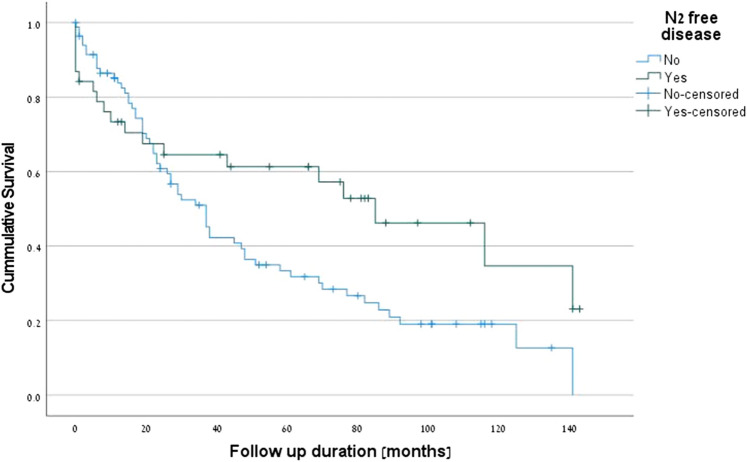
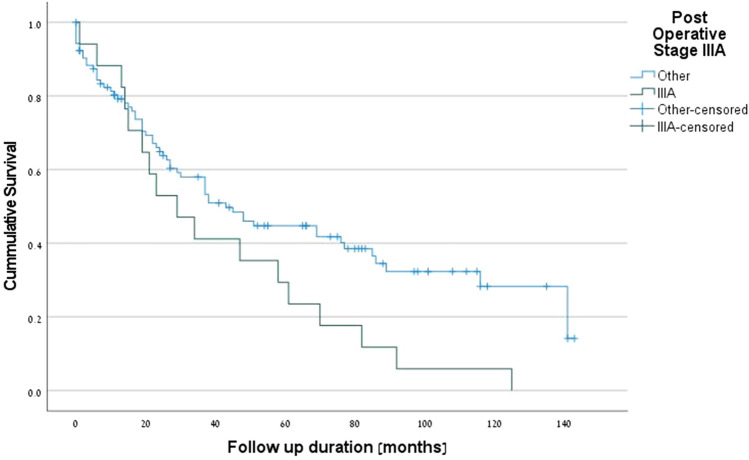
The aim of this study was to identify predictors of postoperative outcome and survival of locally advanced non-small cell lung carcinoma (NSCLC) resections after neoadjuvant chemotherapy or chemoradiation. Medical records of all patients with clinical stage III potentially resectable NSCLC initially treated by neoadjuvant chemotherapy or chemoradiation followed by major pulmonary resections were retrieved from the databases of four Israeli Medical Centers between 1999 to 2019. The 124 suitable patients included, 86 males (69.4%) and 38 females (30.6%), with an average age of 64.2 years (range 37-82) and an average hospital stay of 12.6 days (range 5-123). Complete resection was achieved in 92.7% of the patients, while complete pathologic response was achieved in 35.5%. The overall readmission rate was 16.1%. The overall 5-year survival rate was 47.9%. One patient (0.8%) had local recurrence. Postoperative complications were reported in 49.2% of the patients, mainly atrial fibrillation (15.9%) and pneumonia (13.7%), empyema (10.3%), and early bronchopleural fistula (7.3%). The early in-hospital mortality rate was 6.5%, and the 6-month mortality rate was 5.6%. Pre-neoadjuvant bulky mediastinal disease (lymph nodes > 20 mm) (p = 0.034), persistent postoperative N2 disease (p = 0.016), R1 resection (p = 0.027), preoperative N2 multistation disease (p = 0.053) and postoperative stage IIIA (p = 0.001) emerged as negative predictive factors for survival. Our findings demonstrate that neoadjuvant chemotherapy or chemoradiation in locally advanced potentially resectable NSCLC, followed by major pulmonary resection, is a beneficial approach in selected cases.
本研究旨在确定新辅助化疗或放化疗后局部晚期非小细胞肺癌(NSCLC)切除术的术后结果和生存的预测因素。从 1999 年至 2019 年,从以色列四家医疗中心的数据库中检索到所有接受新辅助化疗或放化疗后行主要肺切除术的临床 III 期可切除 NSCLC 初始治疗的患者的病历。124 例合适的患者包括 86 名男性(69.4%)和 38 名女性(30.6%),平均年龄为 64.2 岁(37-82 岁),平均住院时间为 12.6 天(5-123 天)。92.7%的患者实现了完全切除,而完全病理缓解率为 35.5%。总体再入院率为 16.1%。总体 5 年生存率为 47.9%。1 例患者(0.8%)发生局部复发。49.2%的患者出现术后并发症,主要为心房颤动(15.9%)和肺炎(13.7%)、脓胸(10.3%)和早期支气管胸膜瘘(7.3%)。院内早期死亡率为 6.5%,6 个月死亡率为 5.6%。新辅助治疗时纵隔大病灶(淋巴结>20mm)(p=0.034)、术后持续性 N2 期疾病(p=0.016)、R1 切除(p=0.027)、术前 N2 多站疾病(p=0.053)和术后 IIIA 期(p=0.001)是生存的负预测因素。我们的研究结果表明,在局部晚期可切除 NSCLC 患者中,新辅助化疗或放化疗后行主要肺切除术是一种有益的方法,适用于某些特定病例。