Department of Health Policy and Management, Rollins School of Public Health, Emory University, 1518 Clifton Rd NE, Atlanta, GA, 30322, USA.
Center for Reproductive Health Research in the Southeast (RISE), Emory University, 1518 Clifton Rd NE, Atlanta, GA, 30322, USA.
BMC Health Serv Res. 2021 Oct 22;21(1):1139. doi: 10.1186/s12913-021-07165-x.
To examine racial/ethnic and educational inequities in the relationship between state-level restrictive abortion policies and adverse birth outcomes from 2005 to 2015 in the United States.
Using a state-level abortion restrictiveness index comprised of 18 restrictive abortion policies, we conducted a retrospective longitudinal analysis examining whether race/ethnicity and education level moderated the relationship between the restrictiveness index and individual-level probabilities of preterm birth (PTB) and low birthweight (LBW). Data were obtained from the 2005-2015 National Center for Health Statistics Period Linked Live Birth-Infant Death Files and analyzed with linear probability models adjusted for individual- and state-level characteristics and state and year fixed-effects.
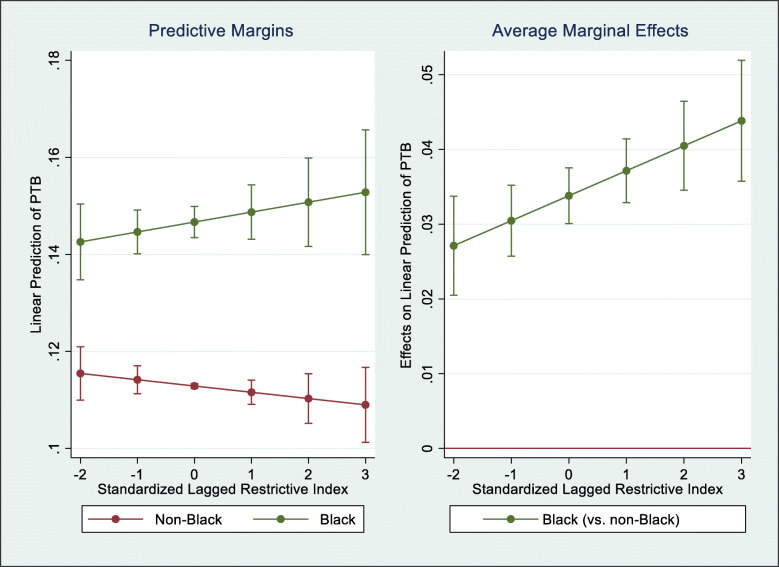
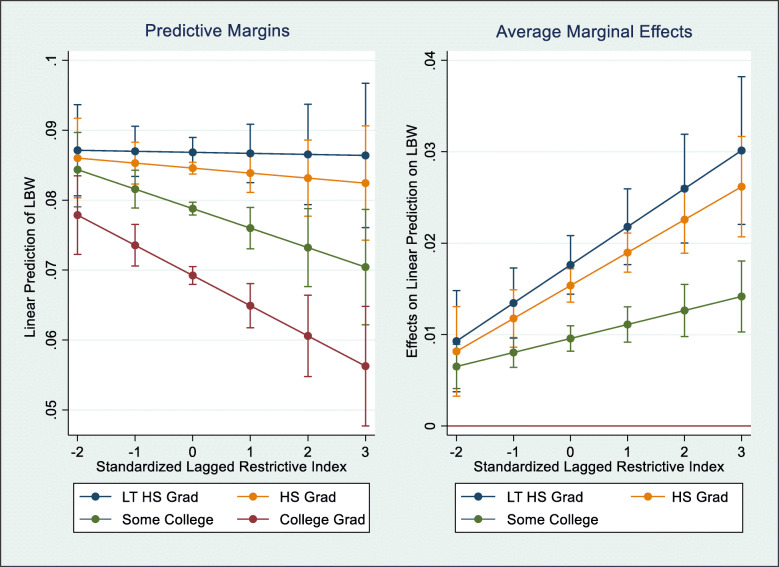
Among 2,250,000 live births, 269,253 (12.0%) were PTBs and 182,960 (8.1%) were LBW. On average, states had approximately seven restrictive abortion policies enacted from 2005 to 2015. Black individuals experienced increased probability of PTB with additional exposure to restrictive abortion policies compared to non-Black individuals. Similarly, those with less than a college degree experienced increased probability of LBW with additional exposure to restrictive abortion policies compared to college graduates. For all analyses, inequities worsened as state environments grew increasingly restrictive.
Findings demonstrate that Black individuals at all educational levels and those with fewer years of education disproportionately experienced adverse birth outcomes associated with restrictive abortion policies. Restrictive abortion policies may compound existing racial/ethnic, socioeconomic, and intersecting racial/ethnic and socioeconomic perinatal and infant health inequities.
本研究旨在考察 2005 年至 2015 年期间,美国各州级限制堕胎政策与不良分娩结局之间的关系中存在的种族/民族和教育不平等现象。
本研究采用了一个由 18 项限制堕胎政策组成的州级堕胎限制指数,通过回顾性纵向分析,考察了种族/民族和教育水平是否调节了限制指数与个体早产(PTB)和低出生体重(LBW)概率之间的关系。数据来源于 2005 年至 2015 年国家卫生统计中心的连续生命-婴儿死亡档案,并使用线性概率模型进行分析,调整了个体和州级特征以及州和年份固定效应。
在 225 万例活产中,269253 例(12.0%)为早产,182960 例(8.1%)为低出生体重。平均而言,各州在 2005 年至 2015 年期间颁布了大约 7 项限制堕胎政策。与非黑人个体相比,黑人个体接触更多的限制堕胎政策会增加早产的概率。同样,与大学毕业生相比,未受过大学教育的个体接触更多的限制堕胎政策会增加低出生体重的概率。在所有分析中,随着州环境的日益限制,不平等现象加剧。
研究结果表明,所有教育水平的黑人个体以及受教育程度较低的个体不成比例地经历了与限制堕胎政策相关的不良分娩结局。限制堕胎政策可能会加剧现有的种族/民族、社会经济以及种族/民族和社会经济交叉的围产期和婴儿健康不平等现象。