Department of Infectious Diseases, Peter MacCallum Cancer Centre, Melbourne, Victoria, Australia; NHMRC National Centre for Infections in Cancer, Sir Peter MacCallum Department of Oncology, University of Melbourne, Parkville, Victoria, Australia; The Paediatric Integrated Cancer Service, Parkville, Victoria State Government, Australia; Infection Diseases Unit, Department of General Medicine, Royal Children's Hospital, Parkville, Victoria, Australia; Infection and Immunity Theme, Murdoch Children's Research Institute, Parkville, Australia.
Paediatric Hematology and Oncology, Department of Paediatrics, Inselspital, Bern University Hospital, Bern, Switzerland; Kinderaerzte KurWerk, Burgdorf, Switzerland.
Eur J Cancer. 2021 Dec;159:78-86. doi: 10.1016/j.ejca.2021.09.027. Epub 2021 Oct 9.
There are limited data on SARS-CoV-2 (COVID-19) infection in children with cancer or after haematopoietic stem cell transplant (HSCT). We describe the severity and outcomes of SARS-COV-2 in these patients and identify factors associated with severe disease.
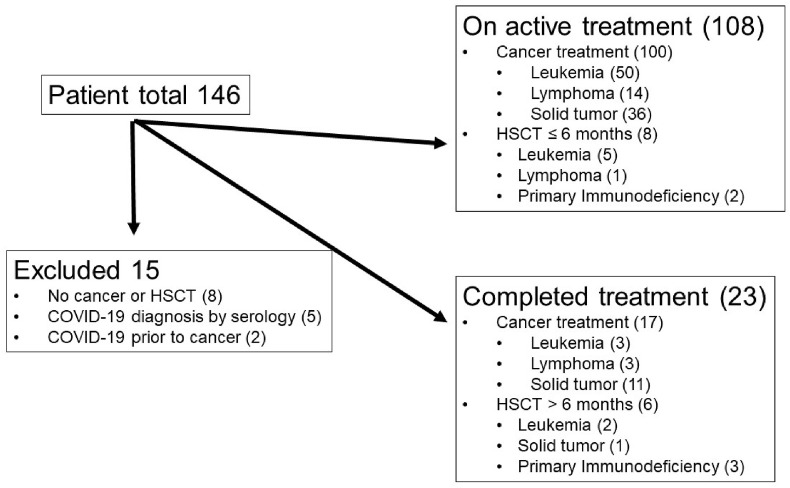
This was a multinational, observational study of children (aged <19 years) with cancer or HSCT and SARS-CoV-2 confirmed by polymerase chain reaction. COVID-19 was classified as asymptomatic, mild, moderate, severe or critical (≥1 organ support). Exact polytomous regression was used to determine the relationship between clinical variables and disease severity.
One hundred and thirty-one patients with COVID-19 across 10 countries were identified (median age 8 years). Seventy-eight (60%) had leukaemia/lymphoma, 48 (37%) had solid tumour and five had primary immunodeficiency and HSCT. Fever (71%), cough (47%) and coryza (29%) were the most frequent symptoms. The median duration of detectable virus was 16 days (range, 1-79 days). Forty-nine patients (37%) were hospitalised for COVID-19 symptoms, and 15 (11%) required intensive care unit-level care. Chemotherapy was delayed/modified in 35% of patients. COVID-19 was asymptomatic in 32% of patients, mild in 47%, moderate in 8%, severe in 4% and critical in 9%. In 124 patients (95%), a full recovery was documented, and four (3%) died due to COVID-19. Any comorbidity (odds ratio, 2.94; 95% confidence interval [CI], 1.81-5.21), any coinfection (1.74; 95% CI 1.03-3.03) and severe baseline neutropenia (1.82; 95% CI 1.13-3.09) were independently and significantly associated with increasing disease severity.
Although most children with cancer had asymptomatic/mild disease, 13% had severe COVID-19 and 3% died. Comorbidity, coinfection and neutropenia may increase the risk of severe disease. Our data may help management decisions in this vulnerable population.
关于患有癌症或接受过造血干细胞移植(HSCT)的儿童中 SARS-CoV-2(COVID-19)感染的数据有限。我们描述了这些患者中 SARS-COV-2 的严重程度和结局,并确定了与严重疾病相关的因素。
这是一项针对患有癌症或接受过 HSCT 且通过聚合酶链反应确认 SARS-CoV-2 感染的儿童(年龄<19 岁)的多中心、观察性研究。COVID-19 分为无症状、轻度、中度、重度或危重(≥1 个器官支持)。使用精确多项回归来确定临床变量与疾病严重程度之间的关系。
在 10 个国家发现了 131 例 COVID-19 患儿(中位年龄 8 岁)。78 例(60%)患有白血病/淋巴瘤,48 例(37%)患有实体瘤,5 例患有原发性免疫缺陷和 HSCT。最常见的症状是发热(71%)、咳嗽(47%)和鼻塞(29%)。可检测病毒的中位持续时间为 16 天(范围,1-79 天)。49 例(37%)因 COVID-19 症状住院,15 例(11%)需要重症监护病房级别的护理。35%的患者化疗延迟/改变。32%的患者 COVID-19 无症状,47%为轻度,8%为中度,4%为重度,9%为危重。在 124 例(95%)患者中,完全康复得到证实,4 例(3%)因 COVID-19 死亡。任何合并症(优势比,2.94;95%置信区间[CI],1.81-5.21)、任何合并感染(1.74;95%CI 1.03-3.03)和严重基线中性粒细胞减少症(1.82;95%CI 1.13-3.09)与疾病严重程度增加独立且显著相关。
尽管大多数患有癌症的儿童患有无症状/轻度疾病,但仍有 13%患有严重 COVID-19,3%死亡。合并症、合并感染和中性粒细胞减少症可能会增加发生严重疾病的风险。我们的数据可能有助于管理决策在这一脆弱人群。