Irschik Stefan, Veljkovic Jelena, Golej Johann, Schlager Gerald, Brandt Jennifer B, Krall Christoph, Hermon Michael
Division of Neonatology, Pediatric Intensive Care and Neuropediatrics, Medical University of Vienna, Vienna, Austria.
Medical University of Vienna, Vienna, Austria.
Front Pediatr. 2021 Oct 28;9:757822. doi: 10.3389/fped.2021.757822. eCollection 2021.
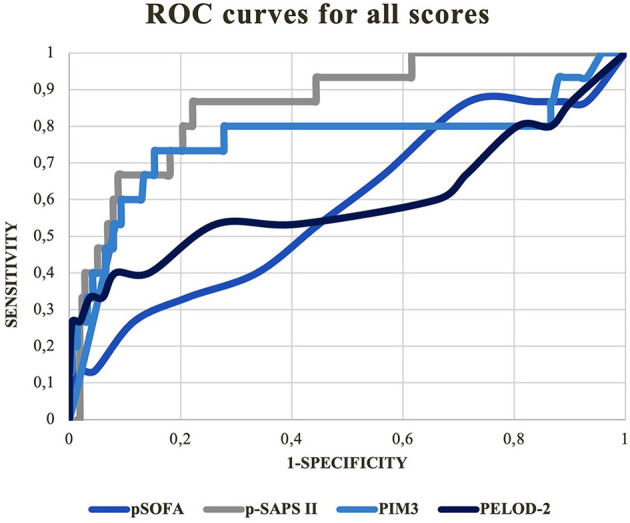
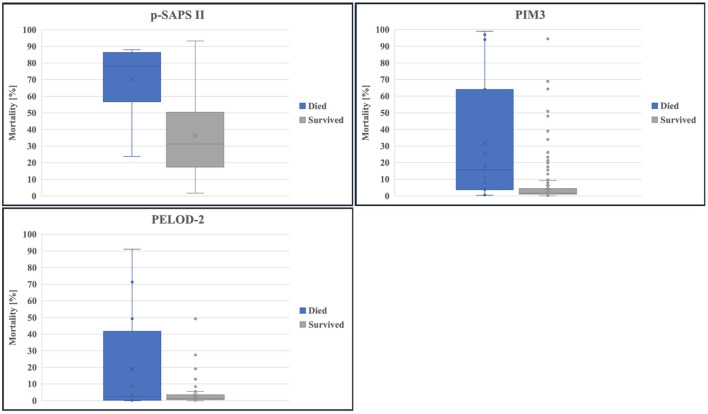
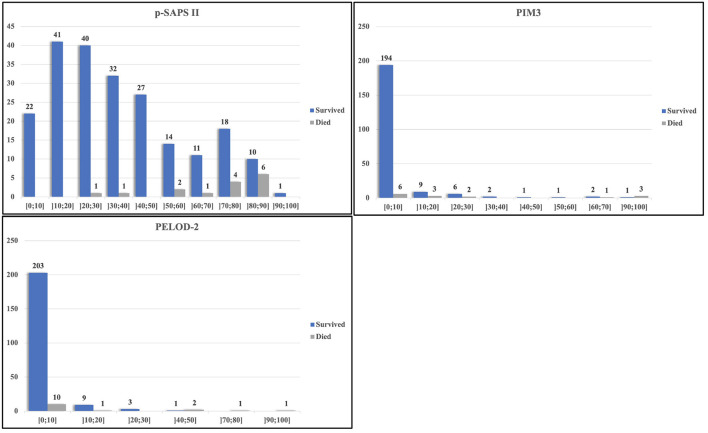
In critical care it is crucial to appropriately assess the risk of mortality for each patient. This is especially relevant in pediatrics, with its need for accurate and repeatable scoring. Aim of this study was to evaluate an age-adapted version of the expanded Simplified Acute Physiology Score II; (p-SAPS II), a repeatable, newly-designed scoring system compared to established scores (Pediatric Sequential Organ Failure Assessment Score/pSOFA, Pediatric Logistic Organ Dysfunction Score-2/PELOD-2 and Pediatric Index of Mortality 3/PIM3). This retrospective cohort pilot study included data collected from patients admitted to the Pediatric Intensive Care Unit (PICU) at the Medical University of Vienna between July 2017 through December 2018. 231 admissions were included, comprising neonates (gestational age of ≥ 37 weeks) and patients up to 18 years of age with a PICU stay longer than 48 h. Mortality risk prediction and discrimination between survivors and non-survivors were the main outcomes of this study. The primary statistical methods for evaluating the performance of each score were the area under the receiver operating characteristic curve (AUROC) and goodness-of-fit test. Highest AUROC curve was calculated for p-SAPS II (AUC = 0.86; 95% CI: 0.77-0.96; < 0.001). This was significantly higher than the AUROCs of PELOD-2/pSOFA but not of PIM3. However, in a logistic regression model including p-SAPS II and PIM3 as covariates, p-SAPS II had a significant effect on the accuracy of prediction ( = 0.003). Nevertheless, according to the goodness-of-fit test for p-SAPS II and PIM3, p-SAPS II overestimated the number of deaths, whereas PIM3 showed acceptable estimations. Repeatability testing showed increasing AUROC values for p-SAPS II throughout the clinical stay (0.96 at day 28) but still no significant difference to PIM 3. The prediction accuracy, although improved over the days and even exceeded PIM 3. The newly-created p-SAPS II performed better than the established PIM3 in terms of discriminating between survivors and non-survivors. Furthermore, p-SAPS II can be assessed repeatably throughout a patient's PICU stay what improves mortality prediction. However, there is still a need to optimize calibration of the score to accurately predict mortality sooner throughout the clinical stay.
在重症监护中,恰当评估每位患者的死亡风险至关重要。这在儿科尤其重要,因为儿科需要准确且可重复的评分。本研究的目的是评估扩展简化急性生理学评分II(p-SAPS II)的年龄适配版本,这是一种可重复的新设计评分系统,并与既定评分(儿科序贯器官衰竭评估评分/pSOFA、儿科逻辑器官功能障碍评分-2/PELOD-2和儿科死亡率指数3/PIM3)进行比较。这项回顾性队列试点研究纳入了2017年7月至2018年12月期间维也纳医科大学儿科重症监护病房(PICU)收治患者的数据。共纳入231例入院患者,包括新生儿(胎龄≥37周)和18岁以下PICU住院时间超过48小时的患者。本研究的主要结果是死亡风险预测以及区分幸存者和非幸存者。评估每个评分性能的主要统计方法是受试者操作特征曲线下面积(AUROC)和拟合优度检验。p-SAPS II的AUROC曲线最高(AUC = 0.86;95%CI:0.77 - 0.96;<0.001)。这显著高于PELOD-2/pSOFA的AUROC,但不高于PIM3。然而,在一个将p-SAPS II和PIM3作为协变量的逻辑回归模型中,p-SAPS II对预测准确性有显著影响(= 0.003)。尽管如此,根据p-SAPS II和PIM3的拟合优度检验,p-SAPS II高估了死亡人数,而PIM3显示出可接受的估计。重复性测试显示,在整个临床住院期间p-SAPS II的AUROC值不断增加(第28天为0.96),但与PIM 3仍无显著差异。预测准确性虽在数天内有所提高,甚至超过了PIM 3。新创建的p-SAPS II在区分幸存者和非幸存者方面比既定的PIM3表现更好。此外,在患者的PICU住院期间可以对p-SAPS II进行重复评估,这提高了死亡风险预测能力。然而,仍需要优化该评分的校准,以便在整个临床住院期间更早地准确预测死亡率。