Nephrology - Dialysis and Kidney Transplantation Unit, University Hospital Mohammed VI, Oujda, University Mohammed First, Oujda, Morocco; Laboratory of Epidemiology, Clinical Research, and Public Health, Medical School, University Mohammed First, Oujda, Morocco.
Nephrology - Dialysis and Kidney Transplantation Unit, University Hospital Mohammed VI, Oujda, University Mohammed First, Oujda, Morocco.
Am J Emerg Med. 2022 Jan;51:374-377. doi: 10.1016/j.ajem.2021.11.013. Epub 2021 Nov 12.
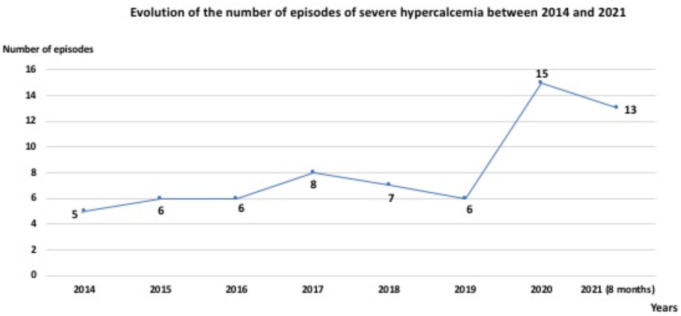
The Covid-19 pandemic has had dramatic consequences on the progression of numerous pathologies, especially neoplastic ones. The orientation of hospital activities toward the care of patients with SARS-Cov2 infection has caused significant delays in the diagnosis and therapy of many other pathologies. What about severe hypercalcemia? The aim of this work was to determine the clinical and biological presentation, etiologies, mortality, and the impact of the Covid-19 pandemic on severe hypercalcemia.
we conducted a retrospective study for 84 months (September 2014 to September 2021) at the Nephrology Unit in University Hospital Mohammed VI, Oujda, Morocco. Included were all adult patients diagnosed with severe hypercalcemia (defined as corrected total serum calcium of >3.5 mmol/l or > 14.0 mg/dl) and who had benefited from one or more hemodialysis sessions.
66 episodes of severe hypercalcemia occurred in 64 patients. The mean age was 57 ± 15 years and 57.6% were female. The mean corrected serum calcium at admission was 16.9 ± 2.1 mg/dl and 33.3% had more than 18.0 mg/dl. Malignancies represented 80.4% of all etiologies. Acute kidney injury was observed in 69.7%. The delta drop in serum calcium 48 h after initiation of medical treatment was 4.64 ± 1.63 mg /dl. Mortality was noted in 14% of all cases. Electrocardiographic abnormalities were observed in 58.3%, 87.5% and 85.7%, respectively, in group 1 (14.0-16.0 mg/dl), group 2 (16.1-18.0 mg/dl), and group 3 (> 18.0 mg/dl) (p = 0.04). The mean serum potassium value was 5.1 ± 1.3, 4.0 ± 1.0, and 3.7 ± 0.7 respectively, in group 1 (14.0-16.0 mg/dl), group 2 (16.1-18.0 mg/dl), and group 3 (> 18.0 mg/dl) (p < 0.001). Newly diagnosed neoplasia, severe hypercalcemia (> 16.0 mg/dl), and mortality have been observed in 15.4% vs. 23.7% (p = 0.31), 25% vs. 50% (p = 0.03), and 35.7% vs. 52.6% (p = 0.13) respectively, in patients before and during the Covid-19 pandemic.
The Covid-19 pandemic caused an increase in both the incidence and severity of hypercalcemia and the hemodialysis practiced in this context remains efficient and safe.
Covid-19 大流行对许多病理学的进展产生了巨大影响,尤其是肿瘤学。医院活动向 SARS-Cov2 感染患者护理的转变导致许多其他病理学的诊断和治疗出现了显著延迟。那么严重高钙血症呢?本研究旨在确定严重高钙血症的临床表现、病因、死亡率以及新冠疫情对严重高钙血症的影响。
我们在摩洛哥乌季达穆罕默德六世大学医院肾脏病科进行了一项回顾性研究,研究时间为 84 个月(2014 年 9 月至 2021 年 9 月)。研究纳入了所有被诊断为严重高钙血症(定义为校正总血清钙>3.5mmol/L 或>14.0mg/dl)并接受过一次或多次血液透析的成年患者。
64 名患者共发生 66 例严重高钙血症发作。平均年龄为 57±15 岁,57.6%为女性。入院时校正血清钙均值为 16.9±2.1mg/dl,33.3%患者钙值>18.0mg/dl。恶性肿瘤占所有病因的 80.4%。69.7%患者发生急性肾损伤。起始药物治疗后 48 小时血清钙降低值为 4.64±1.63mg/dl。所有患者中 14%死亡。心电图异常发生率分别为 58.3%、87.5%和 85.7%,组 1(14.0-16.0mg/dl)、组 2(16.1-18.0mg/dl)和组 3(>18.0mg/dl)(p=0.04)。血清钾值分别为 5.1±1.3、4.0±1.0 和 3.7±0.7,组 1(14.0-16.0mg/dl)、组 2(16.1-18.0mg/dl)和组 3(>18.0mg/dl)(p<0.001)。在新冠疫情前和疫情期间,新诊断的肿瘤、严重高钙血症(>16.0mg/dl)和死亡率分别为 15.4%比 23.7%(p=0.31)、25%比 50%(p=0.03)和 35.7%比 52.6%(p=0.13)。
新冠疫情导致高钙血症的发生率和严重程度均增加,在此背景下进行的血液透析仍然有效且安全。