Gomez Yvan, Balaya Vincent, Lepigeon Karine, Mathevet Patrice, Jacot-Guillarmod Martine
Colposcopy Unit, Women-Mother-Child Department, Lausanne University Hospital, 1011 Lausanne, Switzerland.
Faculty of Biology and Medicine, University of Lausanne, 1015 Lausanne, Switzerland.
J Clin Med. 2021 Nov 15;10(22):5319. doi: 10.3390/jcm10225319.
The aim of this study was to describe the evolution of high-grade cervical dysplasia during pregnancy and the postpartum period and to determine factors associated with dysplasia regression.
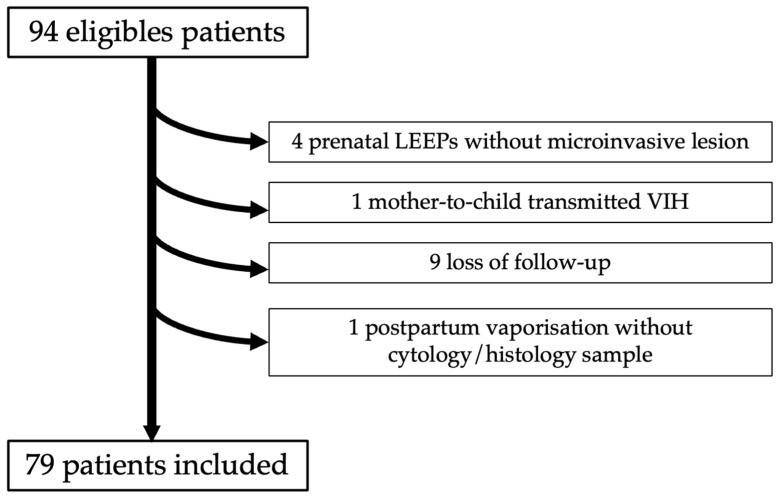
Pregnant patients diagnosed with high-grade lesions were identified in our tertiary hospital center. High-grade lesions were defined either cytologically, by high squamous intraepithelial lesion/atypical squamous cells being unable to exclude HSIL (HSIL/ASC-H), or histologically, with cervical intraepithelial neoplasia (CIN) 2+ (all CIN 2 and CIN 3) during pregnancy. Postpartum regression was defined cytologically or histologically by at least a one-degree reduction in severity from the antepartum diagnosis. A logistic regression model was applied to determine independent predictive factors for high-grade cervical dysplasia regression after delivery.
Between January 2000 and October 2017, 79 patients fulfilled the inclusion criteria and were analyzed. High-grade cervical lesions were diagnosed by cytology in 87% of cases (69/79) and confirmed by histology in 45% of those (31/69). The overall regression rate in our cohort was 43% (34/79). Univariate analysis revealed that parity ( = 0.04), diabetes ( = 0.04) and third trimester cytology ( = 0.009) were associated with dysplasia regression. Nulliparity (OR = 4.35; 95%CI = (1.03-18.42); = 0.046) was identified by multivariate analysis as an independent predictive factor of high-grade dysplasia regression. The presence of HSIL on third-trimester cervical cytology (OR = 0.17; 95%CI = (0.04-0.72); = 0.016) was identified as an independent predictive factor of high-grade dysplasia persistence at postpartum.
Our regression rate was high, at 43%, for high-grade cervical lesions postpartum. Parity status may have an impact on dysplasia regression during pregnancy. A cervical cytology should be performed at the third trimester to identify patients at risk of CIN persistence after delivery. However, larger cohorts are required to confirm these results.
本研究旨在描述妊娠期间及产后高级别宫颈发育异常的演变情况,并确定与发育异常消退相关的因素。
在我们的三级医院中心识别出诊断为高级别病变的孕妇。高级别病变通过细胞学定义为高度鳞状上皮内病变/不能排除高级别鳞状上皮内病变的非典型鳞状细胞(HSIL/ASC-H),或在组织学上定义为妊娠期间宫颈上皮内瘤变(CIN)2+(所有CIN 2和CIN 3)。产后消退通过细胞学或组织学定义为与产前诊断相比严重程度至少降低一级。应用逻辑回归模型确定分娩后高级别宫颈发育异常消退的独立预测因素。
2000年1月至2017年10月,79例患者符合纳入标准并进行了分析。87%的病例(69/79)通过细胞学诊断为高级别宫颈病变,其中45%(31/69)经组织学证实。我们队列中的总体消退率为43%(34/79)。单因素分析显示,产次(P = 0.04)、糖尿病(P = 0.04)和孕晚期细胞学检查(P = 0.009)与发育异常消退相关。多因素分析确定未生育(OR = 4.35;95%CI =(1.03 - 18.42);P = 0.046)是高级别发育异常消退的独立预测因素。孕晚期宫颈细胞学检查存在HSIL(OR = 0.17;95%CI =(0.04 - 0.72);P = 0.016)被确定为产后高级别发育异常持续存在的独立预测因素。
我们的产后高级别宫颈病变消退率较高,为43%。产次状态可能对妊娠期间发育异常的消退有影响。应在孕晚期进行宫颈细胞学检查,以识别分娩后有CIN持续存在风险的患者。然而,需要更大的队列来证实这些结果。