Neuroscience Section, Department of Applied Clinical and Biotechnological Sciences, University of L'Aquila, L'Aquila, Italy.
J Headache Pain. 2021 Nov 27;22(1):144. doi: 10.1186/s10194-021-01361-0.
Transcranial direct current stimulation (tDCS) could counteract the pathophysiological triggers of migraine attacks by modulating cortical excitability. Several pilot randomized controlled trials (RCTs) assessed the efficacy of tDCS for migraine prevention. We reviewed and summarized the state of the art of tDCS protocols for migraine prevention, discussing study results according to the stimulations parameters and patients' populations.
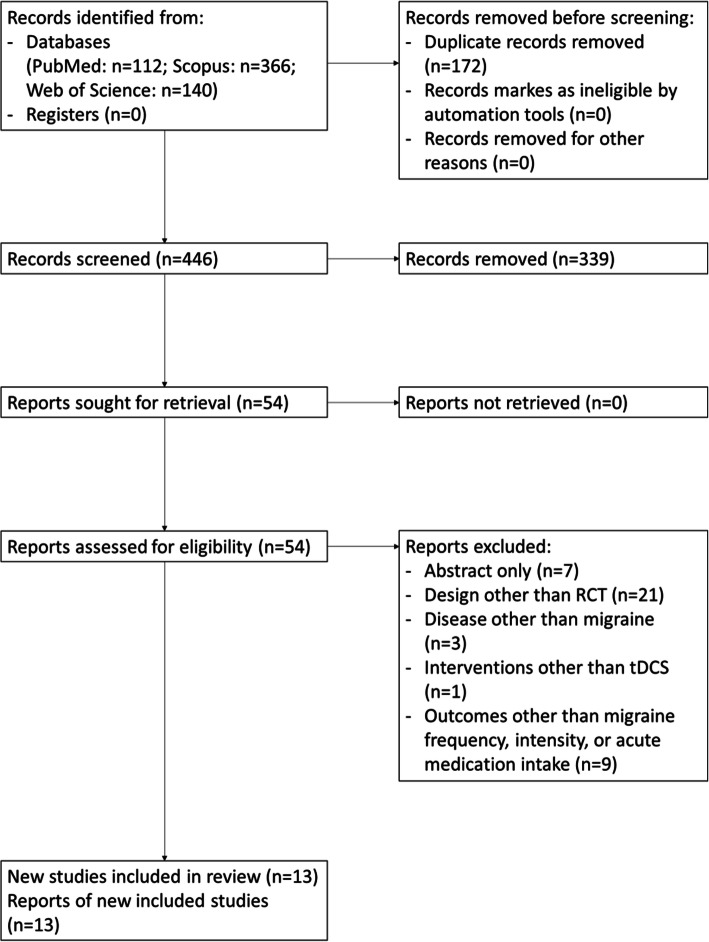
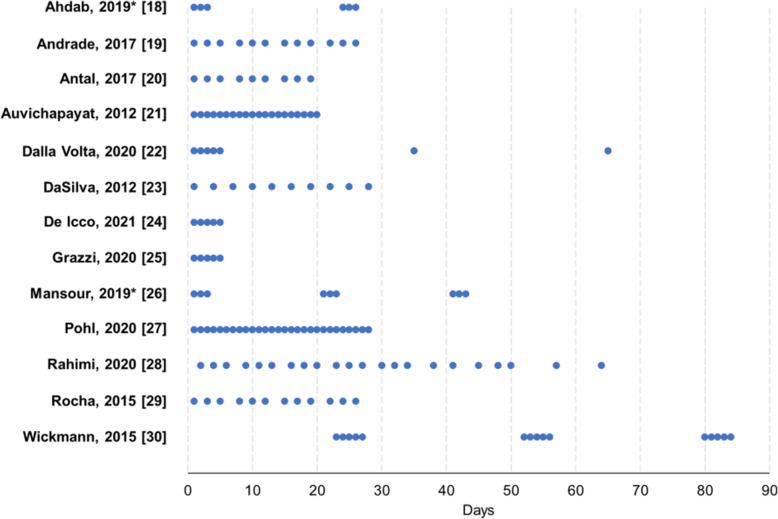
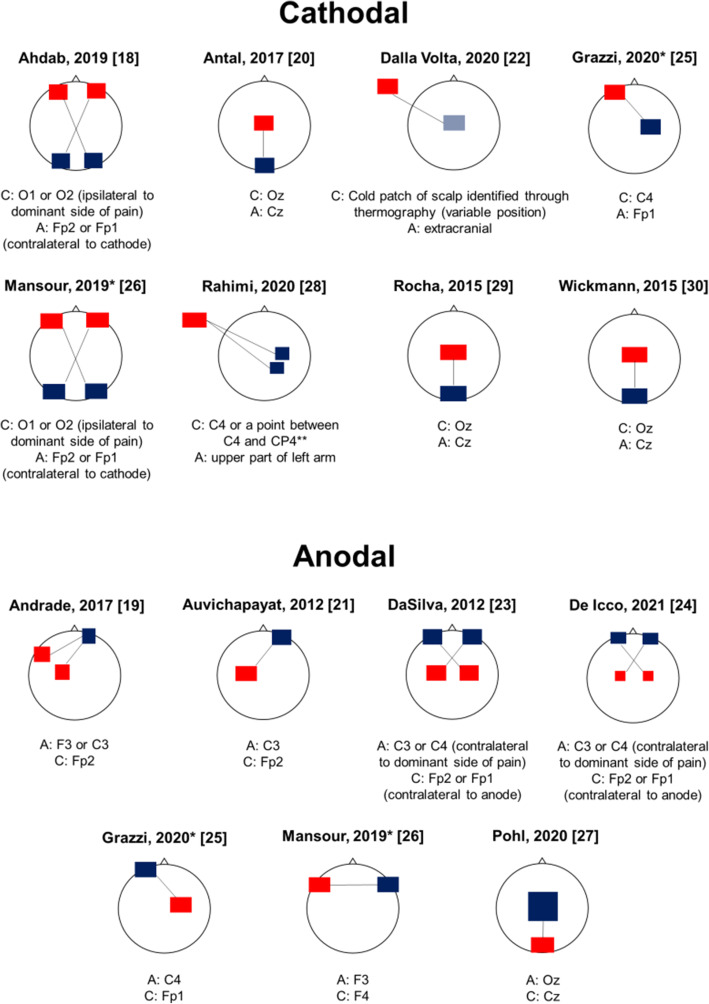
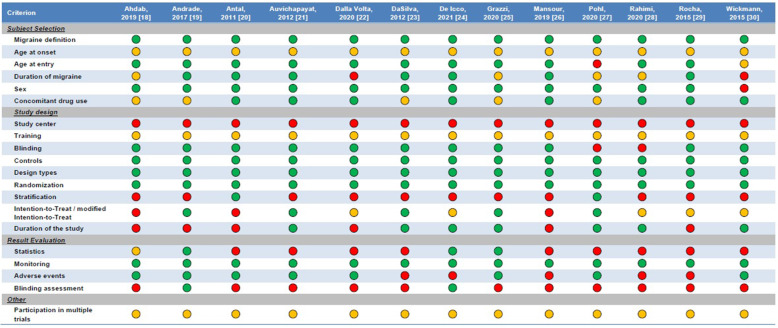
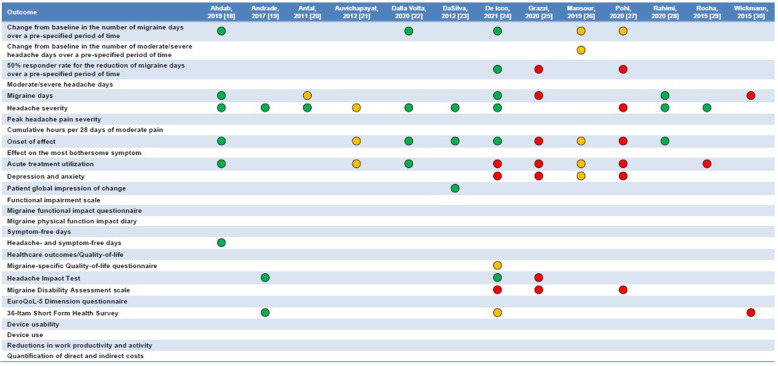
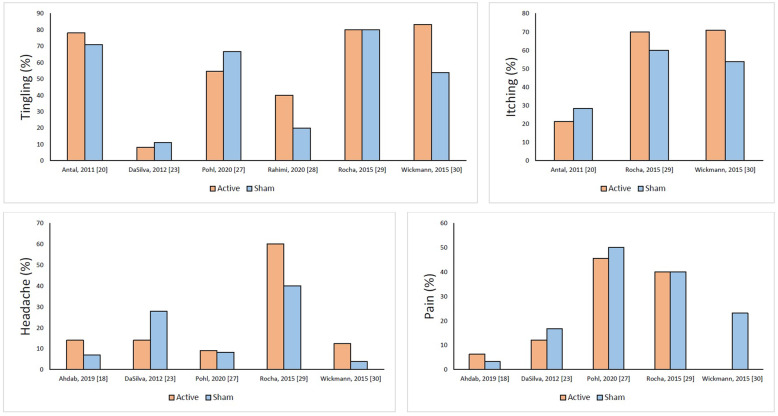
We combined the keywords 'migraine', 'headache', 'transcranial direct current stimulation', and 'tDCS' and searched Pubmed, Scopus, and Web of Science, from the beginning of indexing to June 22, 2021. We only included RCTs comparing the efficacy of active tDCS with sham tDCS to decrease migraine frequency, intensity, and/or acute drug utilization. The risk of bias of each RCT was assessed by using the RoB-2 tool (Cochrane Collaboration). Thirteen RCTs (from 2011 to 2021) were included in the review. The included patients ranged from 13 to 135. RCTs included patients with any migraine (n=3), chronic migraine (n=6), episodic migraine (n=3) or menstrual migraine (n=1). Six RCTs used cathodal and five anodal tDCS, while two RCTs compared the efficacy of both cathodal and anodal tDCS with that of sham. In most of the cathodal stimulation trials, the target areas were the occipital regions, with reference on central or supraorbital areas. In anodal RCTs, the anode was usually placed above the motor cortical areas and the cathode on supraorbital areas. All RCTs adopted repeated sessions (from 5 to 28) at variable intervals, while the follow-up length spanned from 1 day up to 12 months. Efficacy results were variable but overall positive. According to the RoB-2 tool, only four of the 13 RCTs had a low risk of bias, while the others presented some concerns.
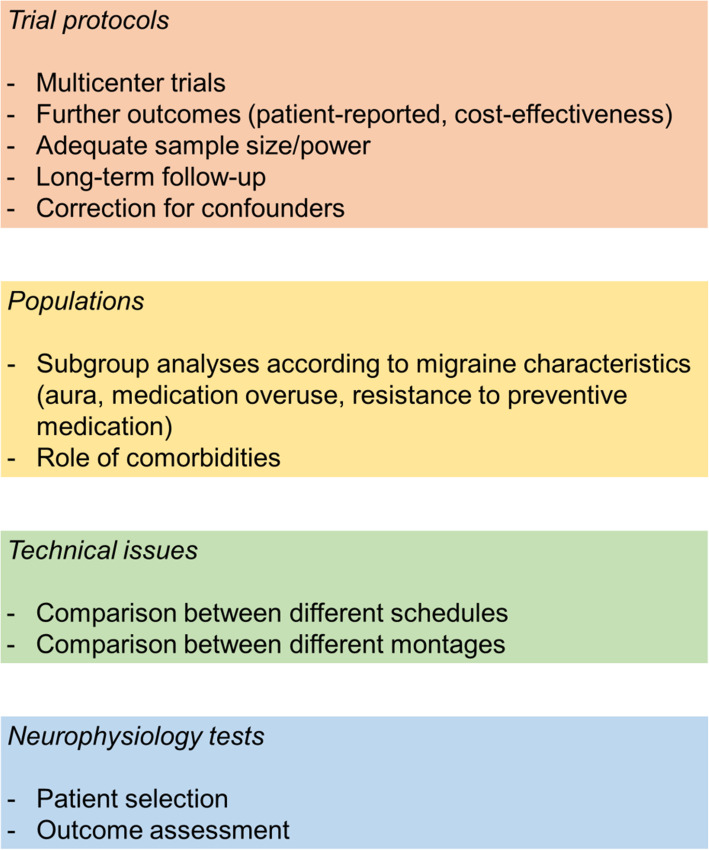
Both anodal and cathodal tDCS are promising for migraine prevention. However, there is a need for larger and rigorous RCTs and standardized procedures. Additionally, the potential benefits and targeted neurostimulation protocols should be assessed for specific subgroups of patients.
经颅直流电刺激(tDCS)可通过调节皮质兴奋性来对抗偏头痛发作的病理生理触发因素。几项初步的随机对照试验(RCT)评估了 tDCS 预防偏头痛的疗效。我们综述并总结了 tDCS 预防偏头痛的方案现状,根据刺激参数和患者人群讨论了研究结果。
我们结合了“偏头痛”、“头痛”、“经颅直流电刺激”和“tDCS”等关键词,在 PubMed、Scopus 和 Web of Science 中进行了搜索,检索时间从索引开始至 2021 年 6 月 22 日。我们仅纳入了比较主动 tDCS 与假刺激 tDCS 降低偏头痛频率、强度和/或急性药物使用的 RCT。使用 RoB-2 工具(Cochrane 协作网)评估每项 RCT 的偏倚风险。综述共纳入了 13 项 RCT(2011 年至 2021 年)。纳入的患者范围从 13 到 135 岁。RCT 纳入了任何偏头痛(n=3)、慢性偏头痛(n=6)、发作性偏头痛(n=3)或经期偏头痛(n=1)患者。6 项 RCT 使用阴极刺激,5 项使用阳极刺激,2 项 RCT 比较了阴极和阳极 tDCS 与假刺激的疗效。在大多数阴极刺激试验中,目标区域是枕叶,以中央或眶上区域为参照。在阳极 RCT 中,阳极通常置于运动皮质区域上方,阴极置于眶上区域。所有 RCT 均采用重复疗程(5 至 28 次),间隔时间不等,随访时间从 1 天至 12 个月不等。疗效结果各不相同,但总体为阳性。根据 RoB-2 工具,13 项 RCT 中仅有 4 项的偏倚风险较低,其余 RCT 存在一些顾虑。
阳极和阴极 tDCS 对偏头痛预防均有一定前景。然而,需要进行更大规模和更严格的 RCT 以及标准化程序。此外,还应评估特定患者亚组的潜在获益和靶向神经刺激方案。