Dipartimento di Medicina Clinica e Chirurgia, Università degli Studi Federico II, Napoli, Italy.
Ematologia Oncologica e Trapianto di Cellule Staminali, Department of Hematology and Developmental Therapeutics, Istituto Nazionale Tumori, Fondazione 'G. Pascale', IRCCS, Via Mariano Semmola 49, 80131, Naples, Italy.
J Transl Med. 2021 Dec 1;19(1):489. doi: 10.1186/s12967-021-03134-4.
Overweight and obese patients with solid tumors receiving anti-programmed cell death-1 (PD-1)/PD-ligand-1(PD-L1) immune checkpoint inhibitors exhibit improved survival and higher risk of immune-related adverse events (irAEs) than those with a normal body mass index (BMI). In classic Hodgkin lymphoma (cHL), the impact of BMI on survival and immune-related toxicity is unknown. We evaluated for the first time associations of BMI with survival and irAEs in patients with relapsed/refractory (RR)-cHL undergoing PD-1 blockade.
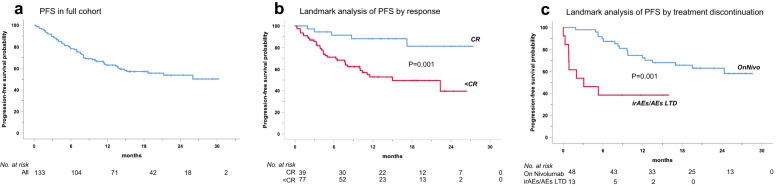
Data from a multicenter study on 133 patients treated with the anti-PD1 antibody nivolumab (July 2015-December 2016) were retrieved from a prospective database. Progression-free (PFS), overall survival (OS), incidence and severity of irAEs according to BMI categories were estimated by Kaplan-Meier method, landmark-analyses and Cox regressions.
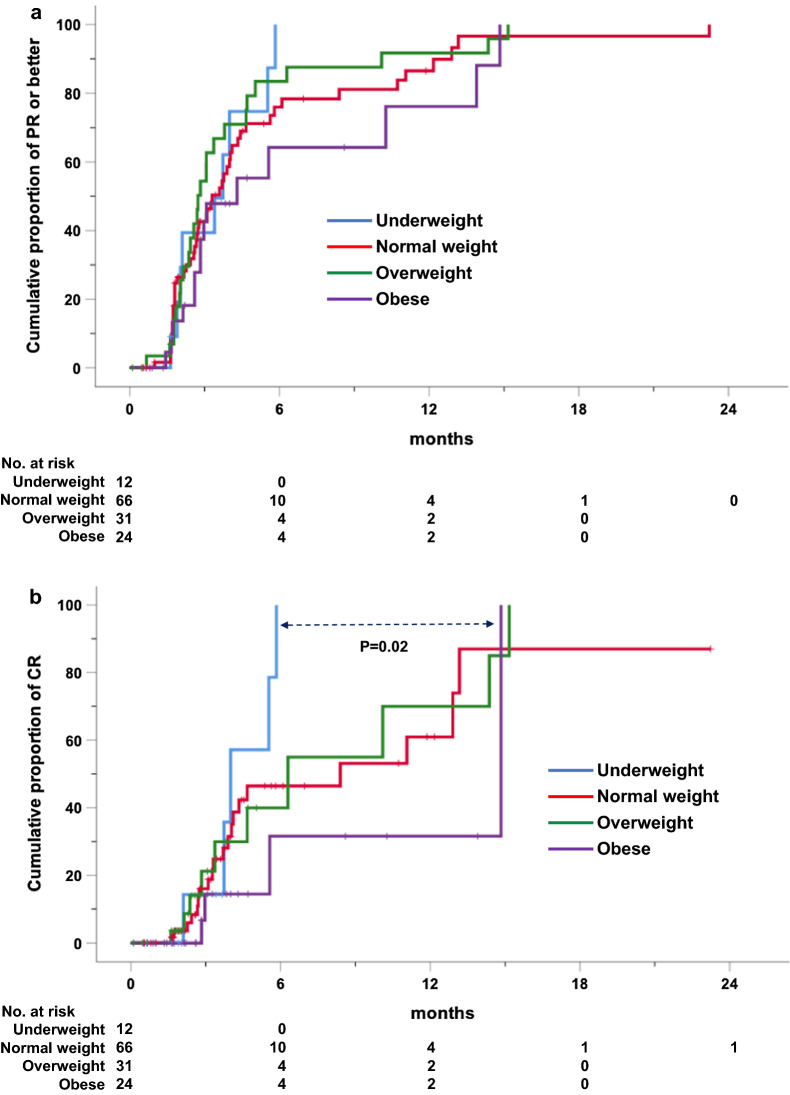
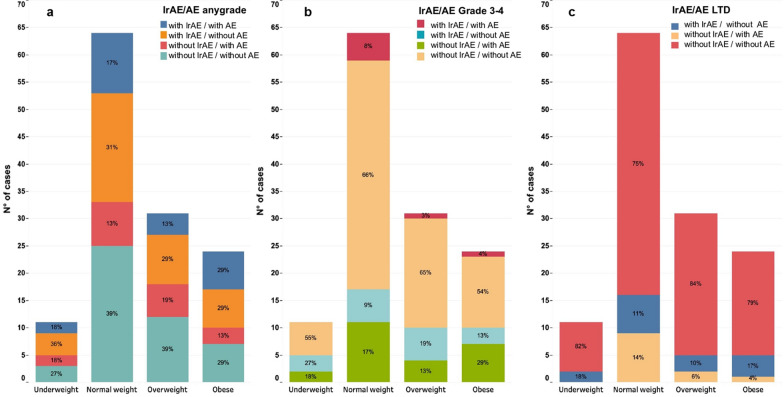
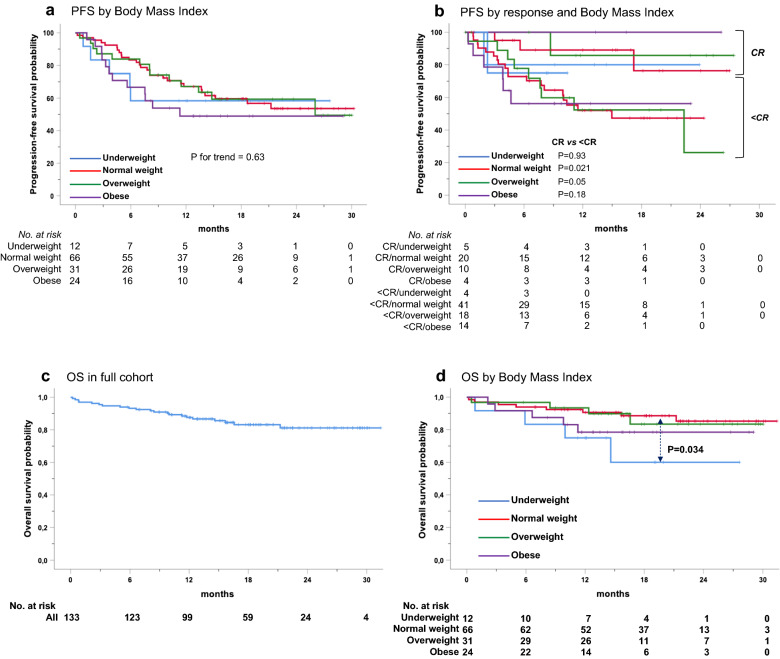
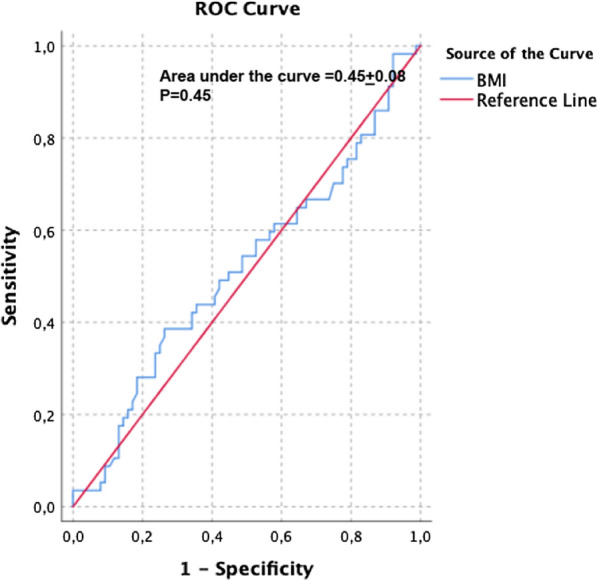
Patients, mostly males (63%, n = 84) with a median age of 35 years (range, 15-82), advanced stage (75%), B symptoms (63%), bulky disease (24%), a median of 4 previous treatments (range, 1-9), received a median of 18 nivolumab doses (range, 1-57). No statistically significant differences across BMI subgroups emerged as to PFS, with 1-year rates of 67.1% for both normal weight (n = 66; 49.6%) and overweight (n = 31; 23.3%) patients. Underweight (n = 12; 9%) and obese (n = 24; 18%) patients had a 1-year PFS of 54.5% and 49%, respectively. In survival analyses, BMI either as a continuous (P = 0.5) or categorical (P for trend = 0.63) variable failed to associate with PFS. Response rates and time-to-response did not cluster in any BMI subset. No BMI-related differences in OS emerged across normal, overweight and obese patients but underweight patients had the worst survival. Occurrence of irAEs of whatever severity did not statistically associate with BMI.
In patients with RR-cHL receiving nivolumab, no statistically significant differences emerged in response rates, PFS and OS across BMI categories of normal weight, overweight and obese. Overweight/obese patients did not display an increased risk of irAEs. The exquisite sensitivity to anti-PD-1 antibodies, the unique cytokine milieu and effector pathways triggered by nivolumab in cHL, may represent biologic 'equalizers' counteracting the immunoregulatory effects of adiposity. Differently from solid tumors, BMI is not associated with treatment efficacy and immune-related toxicity and does not represent a predictive tool for PD-1-targeted immunotherapies in cHL.
与正常体重指数(BMI)相比,接受抗程序性细胞死亡-1(PD-1)/PD-配体-1(PD-L1)免疫检查点抑制剂治疗的患有实体瘤的超重和肥胖患者的生存和发生免疫相关不良事件(irAE)的风险更高。在经典霍奇金淋巴瘤(cHL)中,BMI 对生存和免疫相关毒性的影响尚不清楚。我们首次评估了 BMI 与接受 PD-1 阻断治疗的复发/难治性(RR)-cHL 患者的生存和 irAE 之间的关联。
从一项多中心研究中检索了 133 名接受抗 PD1 抗体纳武单抗(2015 年 7 月至 2016 年 12 月)治疗的患者的数据,这些数据来自一个前瞻性数据库。采用 Kaplan-Meier 法、landmark 分析和 Cox 回归估计 BMI 类别与无进展生存(PFS)、总生存(OS)、irAE 发生率和严重程度的关系。
患者主要为男性(63%,n=84),中位年龄为 35 岁(范围 15-82),晚期(75%),有 B 症状(63%),肿块大(24%),中位数接受了 4 次以前的治疗(范围 1-9),接受了中位数 18 次纳武单抗剂量(范围 1-57)。在 PFS 方面,正常体重(n=66;49.6%)和超重(n=31;23.3%)患者的 1 年 PFS 率均无统计学差异。体重不足(n=12;9%)和肥胖(n=24;18%)患者的 1 年 PFS 率分别为 54.5%和 49%。在生存分析中,BMI 作为连续变量(P=0.5)或分类变量(P 趋势=0.63)均未能与 PFS 相关。反应率和达到反应的时间并未在任何 BMI 亚组中聚集。在正常体重、超重和肥胖患者中,OS 未出现 BMI 相关差异,但体重不足患者的生存最差。irAE 的发生无论严重程度如何,均与 BMI 无统计学关联。
在接受纳武单抗治疗的 RR-cHL 患者中,正常体重、超重和肥胖患者的反应率、PFS 和 OS 无统计学差异。超重/肥胖患者并未显示 irAE 风险增加。纳武单抗在 cHL 中引发的抗 PD-1 抗体的高度敏感性、独特的细胞因子环境和效应途径,可能是对抗肥胖的免疫调节作用的生物学“均衡器”。与实体瘤不同,BMI 与治疗疗效和免疫相关毒性无关,不能作为 cHL 中 PD-1 靶向免疫治疗的预测工具。