Sud Shivani, Botticello Thomas, Niemierko Andrzej, Daly Jillian, Bussiere Marc, Shih Helen A
Department of Radiation Oncology, University of North Carolina Hospitals, Chapel Hill, North Carolina.
Department of Radiation Oncology, Massachusetts General Hospital, Boston, Massachusetts.
Adv Radiat Oncol. 2021 Sep 17;6(6):100806. doi: 10.1016/j.adro.2021.100806. eCollection 2021 Nov-Dec.
To compare the dosimetric differences in stereotactic radiosurgery between use of passively scattered protons (PSRS) versus photons (XSRS) for pituitary adenomas.
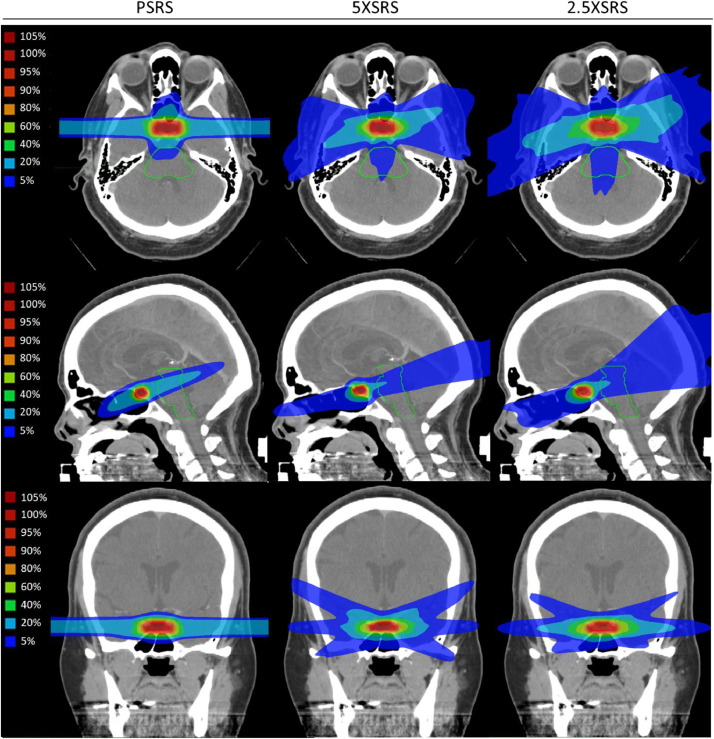
Nine patients with pituitary adenomas were selected among patients receiving single-fraction proton stereotactic radiosurgery (PSRS) between 2016 and 2017. These cases were replanned with XSRS using volumetric-modulated arc therapy with 2.5 mm and 5 mm multileaf collimators (2.5XSRS and 5XSRS, respectively). PSRS was planned with a dedicated single scattering stereotactic proton unit delivered via 3 equally or unequally weighted isocentric fields. XSRS plans were created with optimization to spare organs at risk. Plans were generated using the original total treatment dose delivered in 1 fraction.
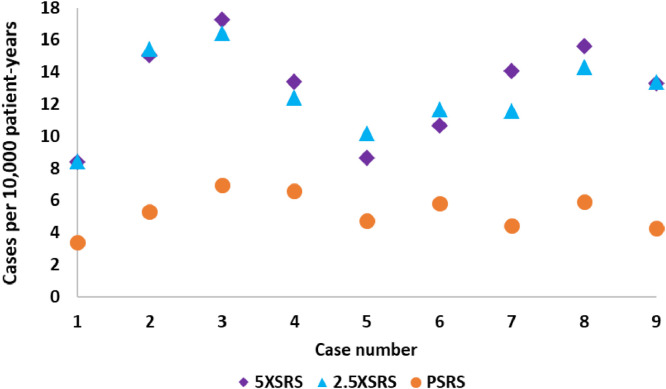
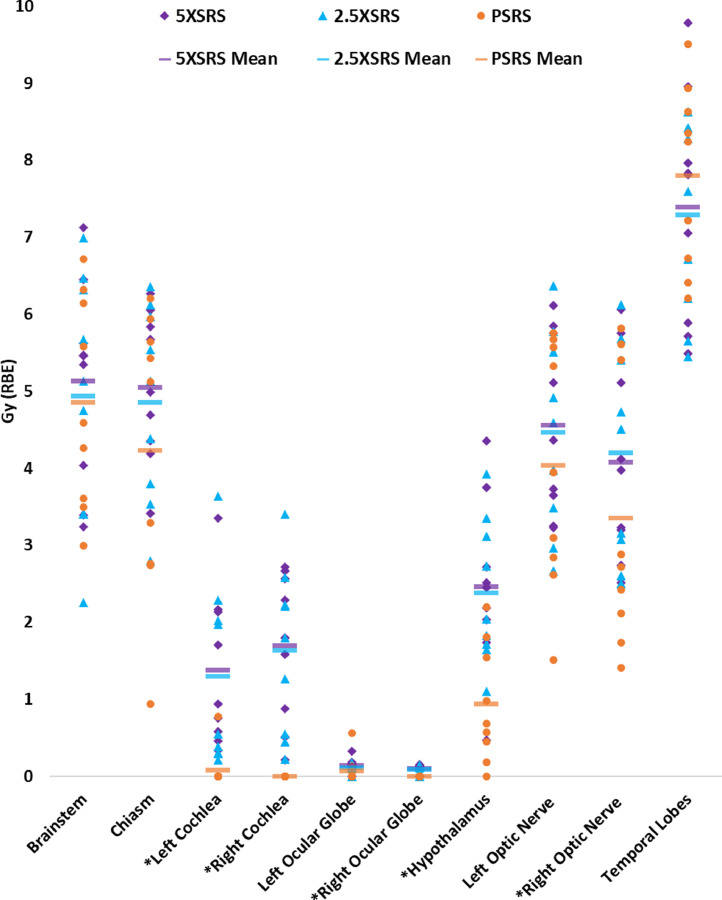
Plans were evaluated for target volume dosimetry and estimated clinical toxicity. There was no significant difference in clinical target volume V100%, V95%, V90% or homogeneity index between treatment modalities. PSRS offered lower maximum dose (Dmax) to organs at risk and equivalent uniform dose (EUD) compared with 5XSRS and 2.5XSRS, respectively, for critical structures including optic nerve (right, Dmax 4.18, 5.32, 5.41; EUD 3.35, 4.08, 4.20) and hypothalamus (Dmax 1.71, 3.94, 3.77; EUD 0.94, 2.47, 2.39; < .05 for PSRS vs 5XSRS and 2.5XSRS). The projected risk of secondary tumors in excess of baseline was lowest for PSRS plans (PSRS 5.28, 5XSRS 12.93, 2.5XSRS 12.66 cases per 10,000 patient-years; = .008 for PSRS vs 5XSRS, PSRS vs 2.5XSRS, and = .77 for 5XSRS vs 2.5XSRS).
We demonstrate that neither modality has empirically superior dosimetry and identify potential clinical advantages as well as limitations of each technique. PSRS, 5XSRS and 2.5XSRS demonstrate comparable target volume dosimetry for pituitary adenoma. PSRS compared with XSRS modalities offers modestly decreased maximum dose and EUD to critical proximal structures and decreases risk of radiation-induced secondary tumors by more than half.
比较垂体腺瘤立体定向放射外科中使用被动散射质子(PSRS)与光子(XSRS)的剂量学差异。
在2016年至2017年接受单次分割质子立体定向放射外科(PSRS)的患者中选择9例垂体腺瘤患者。使用2.5毫米和5毫米多叶准直器的容积调强弧形治疗(分别为2.5XSRS和5XSRS)对这些病例进行XSRS重新计划。PSRS计划通过专用的单散射立体定向质子单元经3个等权重或不等权重的等中心野进行。XSRS计划通过优化以保护危及器官来创建。计划使用单次分割给予的原始总治疗剂量生成。
对计划进行靶区体积剂量学评估和估计的临床毒性评估。不同治疗方式之间临床靶区体积的V100%、V95%、V90%或均匀性指数无显著差异。对于包括视神经(右侧,Dmax分别为4.18、5.32、5.41;EUD分别为3.35、4.08、4.20)和下丘脑(Dmax分别为1.71、3.94、3.77;EUD分别为0.94、2.47、2.39;PSRS与5XSRS和2.5XSRS相比,P <.05)等关键结构,PSRS分别为危及器官提供了更低的最大剂量(Dmax)和等效均匀剂量(EUD)。PSRS计划中超过基线的继发性肿瘤预计风险最低(PSRS为每10,000患者年5.28例,5XSRS为12.93例,2.5XSRS为12.66例;PSRS与5XSRS相比,P = 0.008,PSRS与2.5XSRS相比,P = 0.008,5XSRS与2.5XSRS相比,P = 0.77)。
我们证明两种方式在经验上都没有优越的剂量学表现,并确定了每种技术的潜在临床优势和局限性。PSRS、5XSRS和2.5XSRS在垂体腺瘤的靶区体积剂量学方面表现相当。与XSRS方式相比,PSRS对关键近端结构的最大剂量和EUD略有降低,并将辐射诱发继发性肿瘤的风险降低了一半以上。