Department of Pediatrics, Bayero University/Aminu Kano Teaching Hospital, Kano, Nigeria.
Department of Pediatrics, Hasiya Bayero Pediatric Hospital, Kano, Nigeria.
Lancet Haematol. 2022 Jan;9(1):e26-e37. doi: 10.1016/S2352-3026(21)00368-9.
In high-income countries, standard care for primary stroke prevention in children with sickle cell anaemia and abnormal transcranial Doppler velocities results in a 92% relative risk reduction of strokes but mandates initial monthly blood transfusion. In Africa, where regular blood transfusion is not feasible for most children, we tested the hypothesis that initial moderate-dose compared with low-dose hydroxyurea decreases the incidence of strokes for children with abnormal transcranial Doppler velocities.
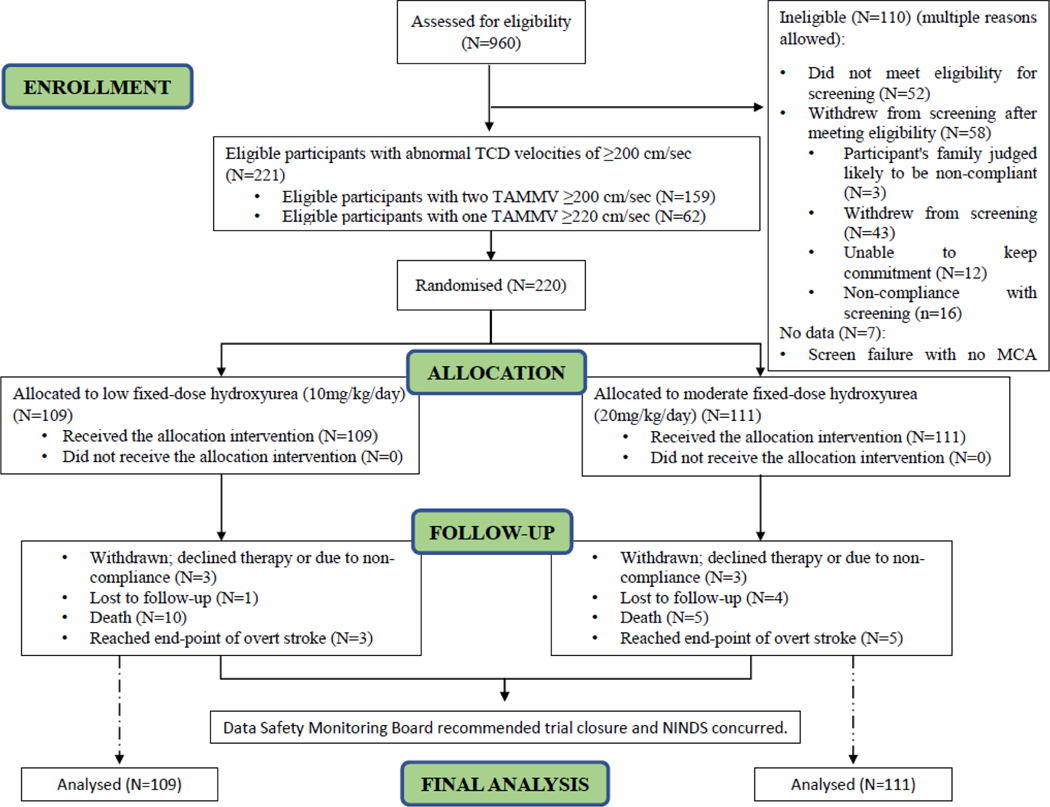
SPRING is a double-blind, parallel-group, randomised, controlled, phase 3 trial of children aged 5-12 years with sickle cell anaemia with abnormal transcranial Doppler velocities conducted at three teaching hospitals in Nigeria. For randomisation, we used a permuted block allocation scheme with block sizes of four, stratified by sex and site. Allocation was concealed from all but the pharmacists and statisticians. Participants were assigned in a 1:1 ratio to low-dose (10 mg/kg per day) or moderate-dose (20 mg/kg per day) oral hydroxyurea taken once daily with monthly clinical evaluation and laboratory monitoring. The primary outcome was initial stroke or transient ischaemic attack, centrally adjudicated. The secondary outcome was all-cause hospitalisation. We used the intention-to-treat population for data analysis. The trial was stopped early for futility after a planned minimum follow-up of 3·0 years to follow-up for participants. This trial was registered with ClinicalTrials.gov, number NCT02560935.
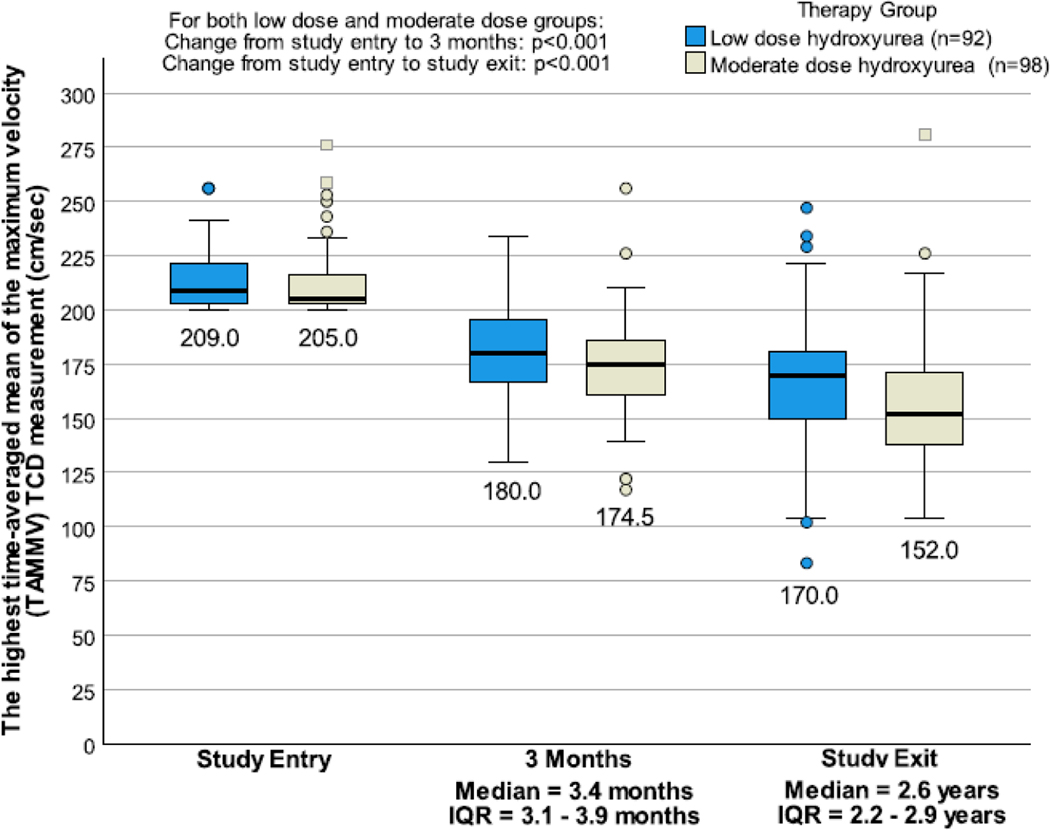
Between Aug 2, 2016, and June 14, 2018, 220 participants (median age 7·2 years [IQR 5·5-8·9]; 114 [52%] female) were randomly allocated and followed for a median of 2·4 years (IQR 2·0-2·8). All participants were Nigerian and were from the following ethnic groups: 179 (82%) people were Hausa, 25 (11%) were Fulani, and 16 (7%) identified as another ethnicity. In the low-dose hydroxyurea group, three (3%) of 109 participants had strokes, with an incidence rate of 1·19 per 100 person-years and in the moderate-dose hydroxyurea group five (5%) of 111 had strokes with an incidence rate of 1·92 per 100 person-years (incidence rate ratio 0·62 [95% CI 0·10-3·20], p=0·77). The incidence rate ratio of hospitalisation for any reason was 1·71 (95% CI 1·15-2·57, p=0·0071), with higher incidence rates per 100 person-years in the low-dose group versus the moderate-dose group (27·43 vs 16·08). No participant had hydroxyurea treatment stopped for myelosuppression.
Compared with low-dose hydroxyurea therapy, participants treated with moderate-dose hydroxyurea had no difference in the stroke incidence rate. However, secondary analyses suggest that the moderate-dose group could lower incidence rates for all-cause hospitalisations. These findings provide an evidence-based guideline for the use of low-dose hydroxyurea therapy for children with sickle cell anaemia at risk of stroke.
National Institute of Neurological Disorders and Stroke.
在高收入国家,针对伴有异常经颅多普勒超声流速的镰状细胞贫血儿童的一级卒中预防的标准治疗可使卒中风险降低 92%,但需要初始每月输血。在非洲,大多数儿童无法进行定期输血,我们检验了这样一个假设,即与低剂量羟脲相比,初始中等剂量羟脲可降低伴有异常经颅多普勒超声流速的儿童卒中的发生率。
SPRING 是一项在尼日利亚三家教学医院进行的、针对 5-12 岁伴有异常经颅多普勒超声流速的镰状细胞贫血儿童的双盲、平行组、随机、对照、3 期试验。采用区组随机化方案,区组大小为 4,按性别和地点分层。分配方案对除药剂师和统计人员以外的所有人均保密。参与者以 1:1 的比例随机分配至低剂量(10mg/kg/天)或中剂量(20mg/kg/天)每日一次的口服羟脲治疗,并进行每月临床评估和实验室监测。主要结局是由中心裁定的首发卒中或短暂性脑缺血发作。次要结局是所有原因的住院治疗。我们使用意向治疗人群进行数据分析。在计划的最低随访 3.0 年以随访参与者后,由于无效而提前终止了试验。这项试验在 ClinicalTrials.gov 注册,编号为 NCT02560935。
2016 年 8 月 2 日至 2018 年 6 月 14 日,220 名参与者(中位年龄 7.2 岁[IQR 5.5-8.9];114 名[52%]为女性)被随机分配并随访中位时间为 2.4 年(IQR 2.0-2.8)。所有参与者均为尼日利亚人,来自以下族裔群体:179 名(82%)参与者为豪萨族,25 名(11%)参与者为富拉尼族,16 名(7%)参与者为其他族裔。在低剂量羟脲组中,有 3 名(3%)109 名参与者发生卒中,发生率为 1.19/100 人年,在中剂量羟脲组中,有 5 名(5%)111 名参与者发生卒中,发生率为 1.92/100 人年(发生率比 0.62[95%CI 0.10-3.20],p=0.77)。任何原因导致的住院治疗发生率比值为 1.71(95%CI 1.15-2.57,p=0.0071),低剂量组的发生率高于中剂量组(27.43 比 16.08)。没有参与者因骨髓抑制而停止羟脲治疗。
与低剂量羟脲治疗相比,接受中剂量羟脲治疗的参与者卒中发生率没有差异。然而,二次分析表明,中剂量组可能会降低所有原因住院治疗的发生率。这些发现为患有镰状细胞贫血且有卒中风险的儿童提供了低剂量羟脲治疗的循证指南。
美国国立神经病学和中风研究所。