Mohamed Muner M B, Wickman Terrance J, Fogo Agnes B, Velez Juan Carlos Q
Department of Nephrology, Ochsner Clinic Foundation, New Orleans, LA.
Department of Pathology, Microbiology and Immunology, Vanderbilt Medical Center, Nashville, TN.
Ochsner J. 2021 Winter;21(4):395-401. doi: 10.31486/toj.21.0083.
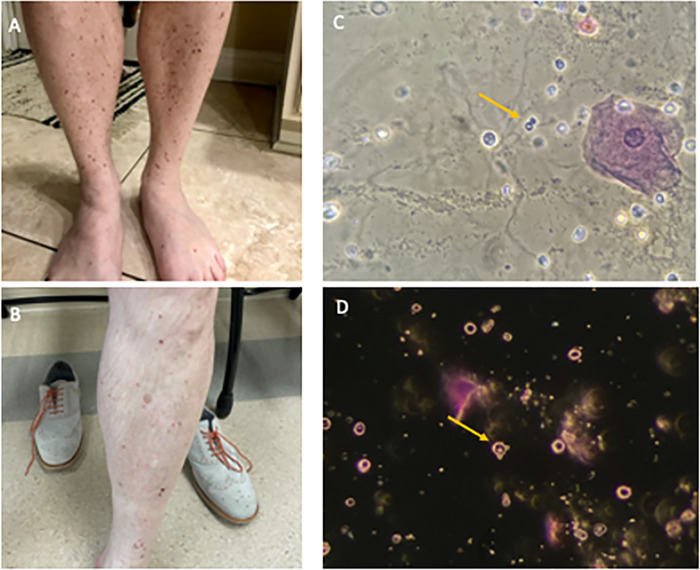
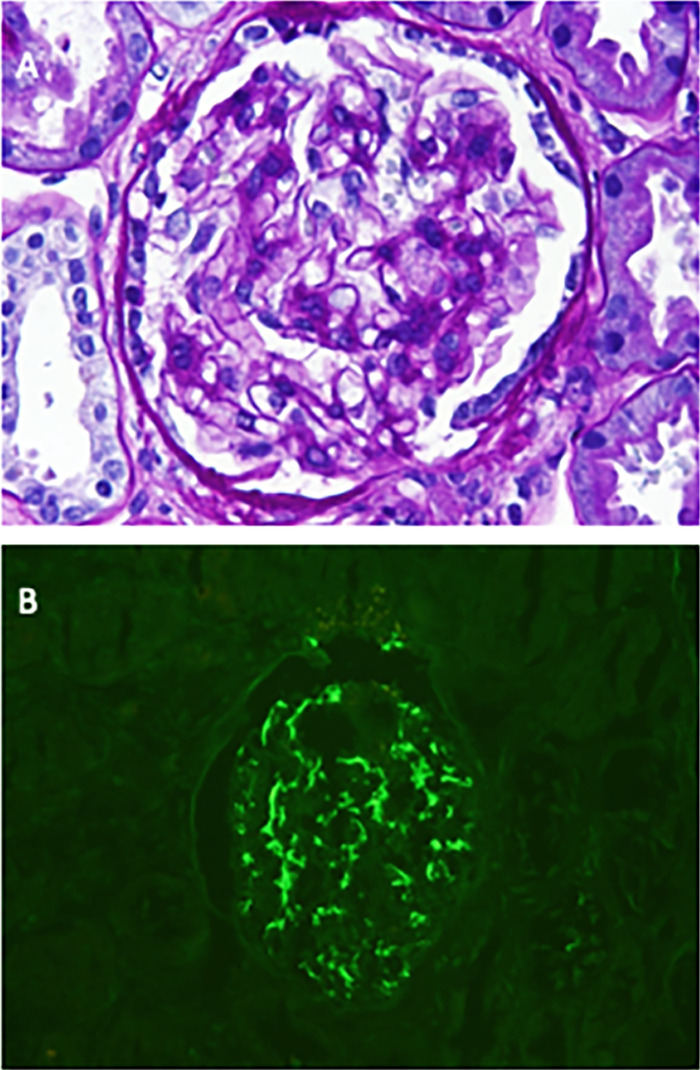
Immunizations have been previously described as potential triggering events for the development of certain glomerular diseases. However, glomerular disease occurrences are being reported after exposure to a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccine. A 50-year-old male presented to a nephrology clinic for evaluation of persistent proteinuria. Six weeks prior to evaluation, the patient had reported developing a rash 2 weeks after receiving the first dose of a SARS-CoV-2 vaccine (BNT162b2 mRNA, Pfizer, Inc). His primary care provider treated the rash with corticosteroids, leading to partial improvement of the skin lesions. Three weeks after the first vaccine injection, the patient received his scheduled second vaccine injection. Within 2 days, the rash reappeared. This time, the lesions were more severe in nature. Skin biopsy revealed immunoglobulin A (IgA)-dominant leukocytoclastic vasculitis. After the patient completed 2 weeks of oral corticosteroids, urinalysis revealed proteinuria, and consultation with nephrology was requested. On examination, healing papules were noted on his legs. Serum creatinine 2 weeks after the second dose of vaccine was 0.9 mg/dL. Microscopic examination of the urinary sediment revealed acanthocytes. Urine protein to creatinine ratio 3 weeks after the second dose of vaccine was 1.1 g/day. Serum complements were normal, and all pertinent serology was negative. Kidney biopsy findings were consistent with IgA nephropathy. The clinical presentation and pathologic findings in this case strongly suggest that the Pfizer SARS-CoV-2 vaccine can trigger a clinical syndrome compatible with Henoch-Schönlein purpura. The recurrence of the rash following the second dose argues for a definite causal association by the Naranjo criteria.
免疫接种先前已被描述为某些肾小球疾病发生的潜在触发事件。然而,在接种严重急性呼吸综合征冠状病毒2(SARS-CoV-2)疫苗后,有肾小球疾病发生的报告。一名50岁男性到肾病科门诊评估持续性蛋白尿。在评估前六周,患者报告在接种第一剂SARS-CoV-2疫苗(BNT162b2 mRNA,辉瑞公司)后2周出现皮疹。他的初级保健医生用皮质类固醇治疗皮疹,使皮肤病变部分改善。在第一次疫苗注射后三周,患者接受了预定的第二次疫苗注射。在两天内,皮疹再次出现。这次,病变性质更严重。皮肤活检显示免疫球蛋白A(IgA)为主的白细胞破碎性血管炎。患者完成2周口服皮质类固醇治疗后,尿液分析显示蛋白尿,因此请求肾病科会诊。检查时,发现他的腿部有愈合的丘疹。第二次疫苗接种后2周血清肌酐为0.9mg/dL。尿沉渣显微镜检查发现棘形红细胞。第二次疫苗接种后3周尿蛋白与肌酐比值为1.1g/天。血清补体正常,所有相关血清学检查均为阴性。肾活检结果符合IgA肾病。该病例的临床表现和病理结果强烈提示,辉瑞SARS-CoV-2疫苗可引发与过敏性紫癜相符的临床综合征。第二次接种后皮疹复发,根据纳朗霍标准可确定存在明确的因果关系。