Department of Medicine, Division of General Internal Medicine, University of Colorado Anschutz School of Medicine, Aurora, USA.
Center for Bioethics and Humanities, University of Colorado, Aurora, USA.
J Gen Intern Med. 2022 Oct;37(13):3310-3317. doi: 10.1007/s11606-021-07300-8. Epub 2022 Jan 11.
Approximately 20% of the US population live in states where MAiD is a legal, though highly contentious, practice. Little generalizable data exists on the experiences of MAiD providers who comprise a small, and intentionally hidden, population.
To examine the nature, extent, and consequences of physicians' participation in MAiD.
An anonymous, multi-wave, mailed survey (RR= 55%).
An enriched sample (n=583) of Colorado physicians caring for potential MAiD patients.
Physician willingness, preparedness, and participation in a continuum of MAiD activities. Other outcomes include the effects of providing MAiD and the barriers physicians face related to MAiD.
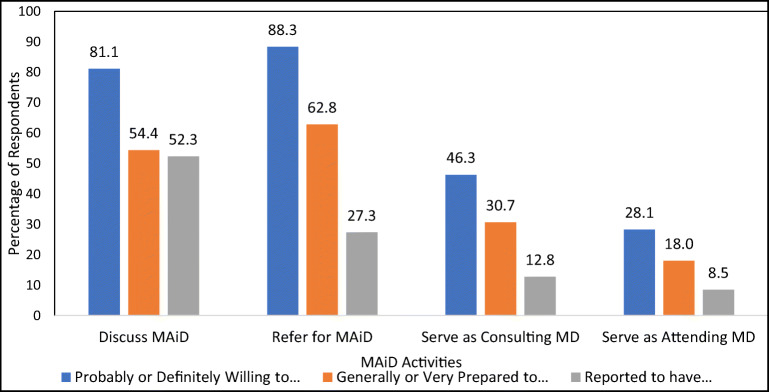
Overall, 81.1% of respondents were willing to discuss MAiD with a patient, 88.3% to refer for MAiD, 46.3% to be a consultant, and 28.1% to be an attending. Fewer felt prepared to discuss MAiD (54.4%), provide a MAiD referral (62.8%), be a consultant (30.7%), or be an attending (18.0%). More than half of respondents (52.3%) had discussed MAiD with a patient, 27.3% provided a MAiD referral, 12.8% had been a MAiD consultant, and 8.5% had been a MAiD attending. Among MAiD consultants and attendings, 75% reported that their most recent MAiD case was emotionally fulfilling and professionally rewarding, though 75% also reported that it was time consuming and 46.9% reported that it was ethically challenging. Common barriers to physician participation in MAiD include lack of knowledge about MAiD (46.8%), the emotional (45.6%) and time (41.7%) investments, and ethical concerns (41.7%).
Many physicians in our sample are both willing and prepared to discuss MAiD with patients and to provide MAiD referrals. Fewer are prepared and willing to serve as an attending or consultant and fewer have provided these services. MAID consultants and attendings largely report the experience to be emotionally fulfilling and professionally rewarding, but all respondents reported multiple barriers to participation.
约 20%的美国人口居住在安乐死合法但极具争议的州。目前很少有关于构成一小部分且故意隐藏的安乐死提供者的经验的可推广数据。
研究医生参与安乐死的性质、范围和后果。
匿名、多波、邮寄调查(RR=55%)。
为潜在的安乐死患者提供护理的科罗拉多州医生的丰富样本(n=583)。
医生参与安乐死的意愿、准备情况和连续性。其他结果包括提供安乐死的影响以及医生面临的与安乐死相关的障碍。
总体而言,81.1%的受访者愿意与患者讨论安乐死,88.3%的受访者愿意转介安乐死,46.3%的受访者愿意担任顾问,28.1%的受访者愿意担任主治医生。较少的人认为他们准备好讨论安乐死(54.4%)、提供安乐死转介(62.8%)、担任顾问(30.7%)或担任主治医生(18.0%)。超过一半的受访者(52.3%)与患者讨论过安乐死,27.3%提供了安乐死转介,12.8%担任过安乐死顾问,8.5%担任过安乐死主治医生。在安乐死顾问和主治医生中,75%的人报告说他们最近的安乐死案例在情感上是令人满意的,在专业上是有益的,尽管 75%的人也报告说这很耗时,46.9%的人报告说这在道德上具有挑战性。医生参与安乐死的常见障碍包括缺乏对安乐死的了解(46.8%)、情感(45.6%)和时间(41.7%)投入以及道德问题(41.7%)。
我们的样本中有许多医生既愿意也准备与患者讨论安乐死并提供安乐死转介。但准备和愿意担任主治医生或顾问的人较少,而且很少有人提供这些服务。安乐死顾问和主治医生大多报告说,他们的经历在情感上是令人满意的,在专业上是有益的,但所有受访者都报告了多个参与障碍。