Shibamori Kosuke, Hashimoto Kohei, Shindo Tetsuya, Tabata Hidetoshi, Kyoda Yuki, Kobayashi Ko, Tanaka Toshiaki, Masumori Naoya
Department of Urology, Sapporo Medical University School of Medicine, Sapporo, Japan.
Curr Urol. 2021 Dec;15(4):198-203. doi: 10.1097/CU9.0000000000000046. Epub 2021 Oct 8.
We investigated the characteristics and outcomes of patients who underwent open partial nephrectomy (OPN) in the minimally invasive approach era.
We retrospectively reviewed 52 patients (55 cases) who underwent OPN from May 2009 to March 2016. We assessed perioperative change in estimated glomerular filtration rate (eGFR), complications, and oncological outcomes. Tumor complexity was evaluated using the R.E.N.A.L nephrometry score (NS) and the modified NS.
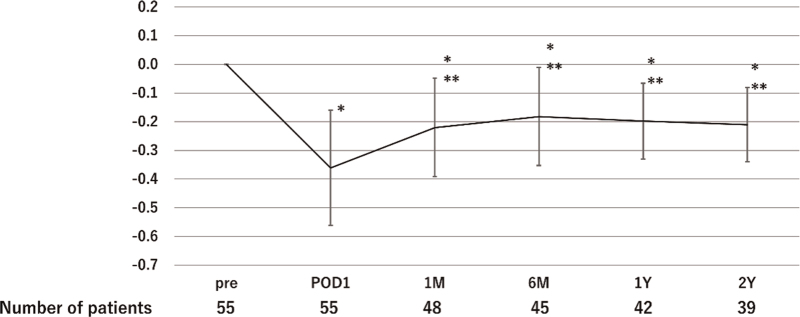
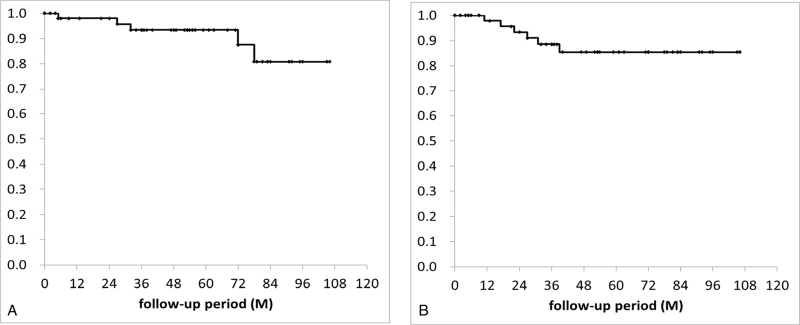
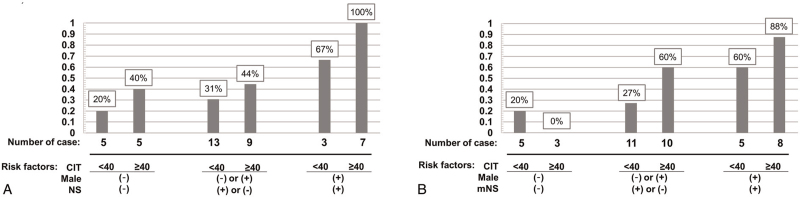
Fifteen cases (27%) had imperative indications and 40 (73%) had elective indications. The elective cases were more likely to have adverse tumor complexity based on NS. The perioperative complication rate defined as a Clavien-Dindo grade ≥IIIa was 11%. The rate of postoperative decline in eGFR at 1 month, 1 year, and 2 years was 22%, 20%, and 21%, respectively. Multivariate analysis revealed that male gender (odds ratio [OR] 11.8, = 0.03), NS ≥9 (OR 13.9, = 0.02), modified NS ≥11 (OR 13.5, = 0.01), and cold ischemic time ≥40 minutes (OR 7.9, = 0.04) were significantly associated with worsening eGFR at 1 year after surgery. During a median follow-up period of 52 months, the 5-year overall survival and recurrence-free survival rates were 93% and 84%, respectively.
OPN is acceptable with regard to oncological outcomes and complications in the minimally invasive surgery era. We propose that OPN should be the preferred approach in cases in which it is technically difficult to preserve maximum renal function via a minimally invasive approach.
我们研究了在微创时代接受开放性部分肾切除术(OPN)患者的特征及预后。
我们回顾性分析了2009年5月至2016年3月期间接受OPN的52例患者(55例手术)。我们评估了估计肾小球滤过率(eGFR)的围手术期变化、并发症及肿瘤学预后。使用R.E.N.A.L肾计量评分(NS)及改良NS评估肿瘤复杂性。
15例(27%)有迫切指征,40例(73%)有择期指征。基于NS,择期病例更可能有不良肿瘤复杂性。定义为Clavien-Dindo分级≥IIIa的围手术期并发症发生率为11%。术后1个月、1年和2年eGFR下降率分别为22%、20%和21%。多因素分析显示,男性(比值比[OR]11.8,P = 0.03)、NS≥9(OR 13.9,P = 0.02)、改良NS≥11(OR 13.5,P = 0.01)及冷缺血时间≥40分钟(OR 7.9,P = 0.04)与术后1年eGFR恶化显著相关。在中位随访期52个月期间,5年总生存率和无复发生存率分别为93%和84%。
在微创手术时代,OPN在肿瘤学预后和并发症方面是可接受的。我们建议,在通过微创方法技术上难以保留最大肾功能的情况下,OPN应是首选方法。