Tuleja Aleksandra, Salvador Dante, Muka Taulant, Bernhard Sarah, Lenz Armando, Baumgartner Iris, Schindewolf Marc
Division of Angiology, Swiss Cardiovascular Center, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland.
Institute of Social and Preventive Medicine (ISPM), University of Bern, Bern, Switzerland.
Blood Adv. 2022 May 24;6(10):3114-3125. doi: 10.1182/bloodadvances.2022007017.
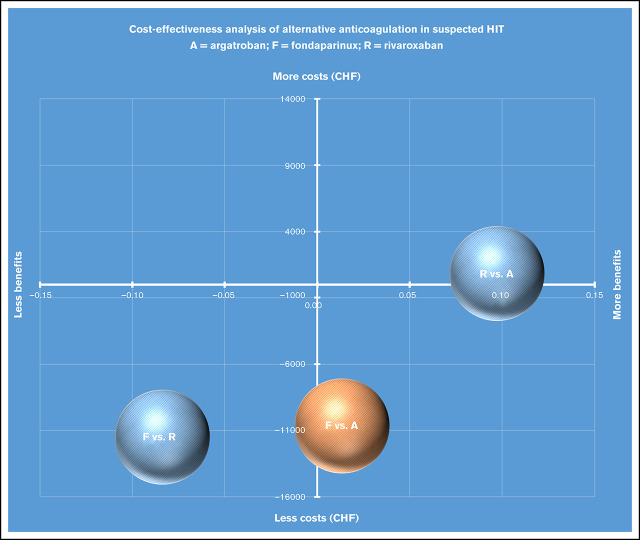
Heparin-induced thrombocytopenia (HIT) is a life-threatening complication associated with high medical costs. Factor Xa inhibitors gradually replace approved treatment with intravenous direct thrombin inhibitors despite their off-label indication, because of easier management and favorable economic profile. Whether they are cost-effective remains unclear. We evaluated the cost-effectiveness of approved and off-label anticoagulants in patients with suspected HIT, based on census data from the largest Swiss hospital between 2015 and 2018. We constructed a decision tree model that reflects important clinical events associated with HIT. Relevant cost data were obtained from the finance department or estimated based on the Swiss-wide cost tariff. We estimated averted adverse events (AEs) and incremental cost-effectiveness ratio as primary outcome parameters. We performed deterministic and probabilistic sensitivity analyses with 2000 simulations to assess the robustness of our results. In the base-case analysis, the total cost of averting 1 AE was 49 565 Swiss francs (CHF) for argatroban, 30 380 CHF for fondaparinux, and 30 610 CHF for rivaroxaban; after adjusting for 4Ts score: 41 152 CHF (argatroban), 27 710 CHF (fondaparinux), and 37 699 CHF (rivaroxaban). Fondaparinux and rivaroxaban were more clinically effective than argatroban, with AEs averted of 0.820, 0.834, and 0.917 for argatroban, fondaparinux, and rivaroxaban, respectively. Treatment with fondaparinux resulted in less cost and more AEs averted, hence dominating argatroban. Results were most sensitive to AE rates and prolongation of stay. Monte Carlo simulations affirmed our base-case analysis. This is the first cost-effectiveness analysis comparing argatroban with fondaparinux and rivaroxaban using primary data. Fondaparinux and rivaroxaban resulted in more averted AEs, but fondaparinux had greater cost savings. Fondaparinux could be a viable alternative to argatroban.
肝素诱导的血小板减少症(HIT)是一种危及生命的并发症,且医疗成本高昂。尽管Xa因子抑制剂的适应证未获批准,但因其管理更简便且经济状况良好,已逐渐取代静脉直接凝血酶抑制剂成为获批治疗药物。其是否具有成本效益尚不清楚。我们基于2015年至2018年瑞士最大医院的普查数据,评估了疑似HIT患者使用获批和未获批抗凝剂的成本效益。我们构建了一个决策树模型,该模型反映了与HIT相关的重要临床事件。相关成本数据来自财务部门或根据瑞士全国成本费率估算。我们将避免的不良事件(AE)和增量成本效益比作为主要结局参数。我们进行了确定性和概率性敏感性分析,并进行了2000次模拟,以评估结果的稳健性。在基础病例分析中,阿加曲班避免1例AE的总成本为49565瑞士法郎(CHF),磺达肝癸钠为30380 CHF,利伐沙班为30610 CHF;根据4Ts评分调整后:阿加曲班为41152 CHF,磺达肝癸钠为27710 CHF,利伐沙班为37699 CHF。磺达肝癸钠和利伐沙班在临床上比阿加曲班更有效,阿加曲班、磺达肝癸钠和利伐沙班避免的AE分别为0.820、0.834和0.917。使用磺达肝癸钠治疗成本更低,避免的AE更多,因此优于阿加曲班。结果对AE发生率和住院时间延长最为敏感。蒙特卡洛模拟证实了我们的基础病例分析。这是首次使用原始数据比较阿加曲班与磺达肝癸钠和利伐沙班成本效益的分析。磺达肝癸钠和利伐沙班避免的AE更多,但磺达肝癸钠节省的成本更多。磺达肝癸钠可能是阿加曲班的可行替代药物。