Wittka Alina, Ketteler Julia, Borgards Lars, Maier Patrick, Herskind Carsten, Jendrossek Verena, Klein Diana
Institute of Cell Biology (Cancer Research), University of Duisburg-Essen, Medical Faculty Essen, Essen, Germany.
Department of Radiation Oncology, University Medical Center Mannheim, Medical Faculty Mannheim, Heidelberg University, Mannheim, Germany.
Front Oncol. 2022 Jan 26;12:802482. doi: 10.3389/fonc.2022.802482. eCollection 2022.
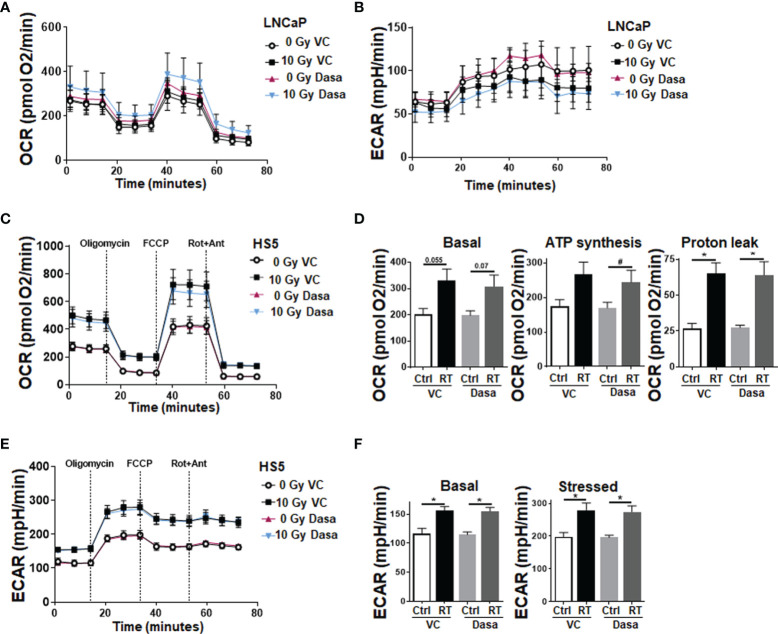
In prostate cancer (PCa), a characteristic stromal-epithelial redistribution of the membrane protein caveolin 1 (CAV1) occurs upon tumor progression, where a gain of CAV1 in the malignant epithelial cells is accompanied by a loss of CAV1 in the tumor stroma, both facts that were correlated with higher Gleason scores, poor prognosis, and pronounced resistance to therapy particularly to radiotherapy (RT). However, it needs to be clarified whether inhibiting the CAV1 gain in the malignant prostate epithelium or limiting the loss of stromal CAV1 would be the better choice for improving PCa therapy, particularly for improving the response to RT; or whether ideally both processes need to be targeted. Concerning the first assumption, we investigated the RT response of LNCaP PCa cells following overexpression of different CAV1 mutants. While CAV1 overexpression generally caused an increased epithelial-to-mesenchymal phenotype in respective LNCaP cells, effects that were accompanied by increasing levels of the 5'-AMP-activated protein kinase (AMPK), a master regulator of cellular homeostasis, only wildtype CAV1 was able to increase the three-dimensional growth of LNCaP spheroids, particularly following RT. Both effects could be limited by an additional treatment with the SRC inhibitor dasatinib, finally resulting in radiosensitization. Using co-cultured (CAV1-expressing) fibroblasts as an approximation to the situation of early PCa it could be revealed that RT itself caused an activated, more tumor-promoting phenotype of stromal fibroblats with an increased an increased metabolic potential, that could not be limited by combined dasatinib treatment. Thus, targeting fibroblasts and/or limiting fibroblast activation, potentially by limiting the loss of stromal CAV1 seems to be absolute for inhibiting the resistance-promoting CAV1-dependent signals of the tumor stroma.
在前列腺癌(PCa)中,随着肿瘤进展,膜蛋白小窝蛋白1(CAV1)会出现特征性的基质 - 上皮重新分布,即恶性上皮细胞中CAV1增加的同时,肿瘤基质中的CAV1减少,这两个事实均与更高的 Gleason 评分、预后不良以及对治疗尤其是放疗(RT)的显著抗性相关。然而,需要明确的是,抑制恶性前列腺上皮中CAV1的增加还是限制基质CAV1的丢失,对于改善PCa治疗,特别是改善对RT的反应,哪个是更好的选择;或者理想情况下是否需要同时针对这两个过程。关于第一个假设,我们研究了不同CAV1突变体过表达后LNCaP前列腺癌细胞的放疗反应。虽然CAV1过表达通常会在相应的LNCaP细胞中导致上皮 - 间充质表型增加,这种效应伴随着细胞内稳态的主要调节因子5'-AMP激活蛋白激酶(AMPK)水平的升高,但只有野生型CAV1能够增加LNCaP球体的三维生长,特别是在放疗后。这两种效应都可以通过额外使用SRC抑制剂达沙替尼来限制,最终导致放射增敏。使用共培养的(表达CAV1的)成纤维细胞来近似早期PCa的情况,结果显示放疗本身会导致基质成纤维细胞具有活化的、更具肿瘤促进性的表型,其代谢潜能增加,而联合使用达沙替尼治疗无法限制这种情况。因此,针对成纤维细胞和/或限制成纤维细胞激活,可能通过限制基质CAV1的丢失,对于抑制肿瘤基质中促进抗性的CAV1依赖性信号似乎是至关重要的。