Service of Thoracic Surgery, University Hospital of Lausanne, Lausanne, Switzerland.
Division of Thoracic and Endocrine Surgery, Geneva University Hospitals and University of Geneva, Geneva, Switzerland.
Interact Cardiovasc Thorac Surg. 2022 Jun 15;35(1). doi: 10.1093/icvts/ivac039.
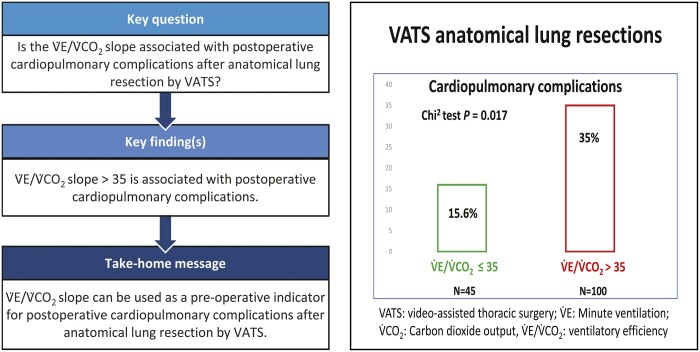
The aim of this study was to identify whether steeper V.E/V. CO2 slope was associated with cardiopulmonary complications (CPC) after anatomical resection by video-assisted thoracic surgery. Long-term survival was analysed as secondary outcome.
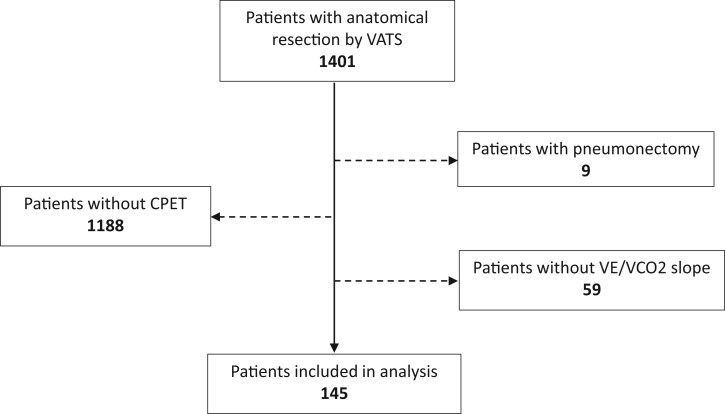
We reviewed the files of all consecutive patients who underwent pulmonary anatomical resections by video-assisted thoracic surgery between January 2010 and October 2020 at the Centre for Thoracic Surgery of Western Switzerland. Logistic regression was used to investigate the risk of CPC associated with the V.E/V.CO2 slope and other possible confounders. Survival was analysed with Kaplan-Meier curves. Risk factors associated with survival were analysed with a Cox proportional hazards model.
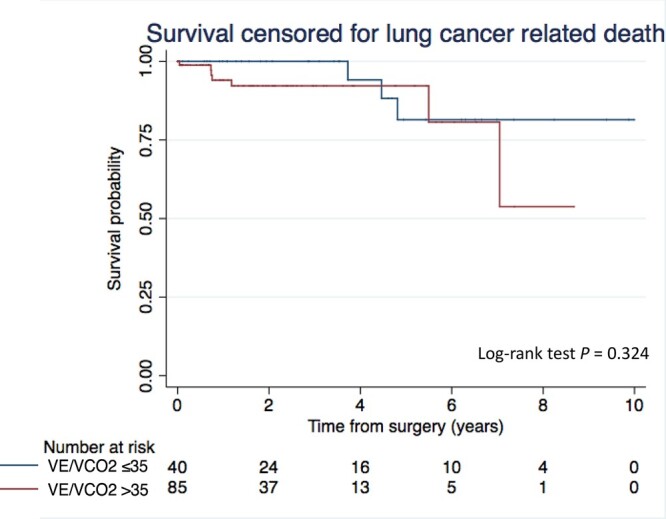
The V.E/V.CO2 slope data were available for 145 patients [F/M: 66/79; mean age (standard deviation): 65.8 (8.9)], which were included in the analysis. Patients underwent anatomical resection [lobectomy (71%) or segmentectomy (29%)] mainly for lung cancer (96%). CPC and all-cause 90-day mortality were 29% and 1%, respectively. The mean (standard deviation) percentage of the predicted V.O2peak was 70% (17). Maximum effort during cardiopulmonary exercise test was reached in only 31% of patients. The V.E/V.CO2 slope (standard deviation) was not different if the maximum effort was reached or not [39 (6) vs 37 (7), P = 0.21]. V.E/V.CO2 slope >35 was associated with an increased risk of CPC (odds ratio 2.9, 95% confidence interval 1.2, 7.2, P = 0.020). V.E/V.CO2 slope >35 was not associated with shorter survival censored for lung cancer-related death.
V . E/V.CO2 slope >35 is significantly associated with postoperative CPC after anatomical resections by video-assisted thoracic surgery.
CLINICAL REGISTRATION NUMBER CER-VD (SWITZERLAND): Project ID: 2021-00620.
本研究旨在确定视频辅助胸腔镜解剖性肺切除术后,呼气末二氧化碳分压与通气比值(V.E/V.CO2 斜率)的陡峭程度是否与心肺并发症(CPC)相关。作为次要结局,我们分析了长期生存率。
我们回顾了 2010 年 1 月至 2020 年 10 月期间,在瑞士西部胸外科中心接受视频辅助胸腔镜解剖性肺切除术的所有连续患者的病历。使用逻辑回归分析 V.E/V.CO2 斜率与 CPC 相关的风险以及其他可能的混杂因素。Kaplan-Meier 曲线分析生存情况。Cox 比例风险模型分析与生存相关的危险因素。
145 例患者(男/女:66/79;平均年龄[标准差]:65.8[8.9])的 V.E/V.CO2 斜率数据可用于分析。患者接受解剖性切除术[肺叶切除术(71%)或肺段切除术(29%)]主要是为了治疗肺癌(96%)。CPC 和全因 90 天死亡率分别为 29%和 1%。预测最大摄氧量(V.O2peak)的平均(标准差)百分比为 70%(17)。仅 31%的患者达到了心肺运动试验的最大努力。达到最大努力与未达到最大努力时的 V.E/V.CO2 斜率(标准差)无差异[39(6)比 37(7),P=0.21]。V.E/V.CO2 斜率>35 与 CPC 风险增加相关(比值比 2.9,95%置信区间 1.2,7.2,P=0.020)。V.E/V.CO2 斜率>35 与未因肺癌相关死亡而被删失的生存时间无相关性。
V.E/V.CO2 斜率>35 与视频辅助胸腔镜解剖性肺切除术后的术后 CPC 显著相关。
临床注册号 CER-VD(瑞士):项目 ID:2021-00620。