Hong Soojung, Daniels Benjamin, van Leeuwen Marina T, Pearson Sallie-Anne, Vajdic Claire M
Centre for Big Data Research in Health, UNSW Sydney, Sydney, Australia.
Division of Oncology-Hematology, Department of Internal Medicine, National Health Insurance Service, Ilsan Hospital, Ilsan-ro 100, Goyang, Republic of Korea.
Discov Oncol. 2022 Jan 20;13(1):6. doi: 10.1007/s12672-022-00468-3.
Clinical trials report systemic hypertension is an adverse effect of vascular signalling pathway inhibitor (VSPi) use. There are limited data from routine clinical practice. We aimed to estimate the real-world incidence and risk factors of new-onset and aggravated hypertension for cancer patients dispensed VSPi in whole-of-population Australian setting.
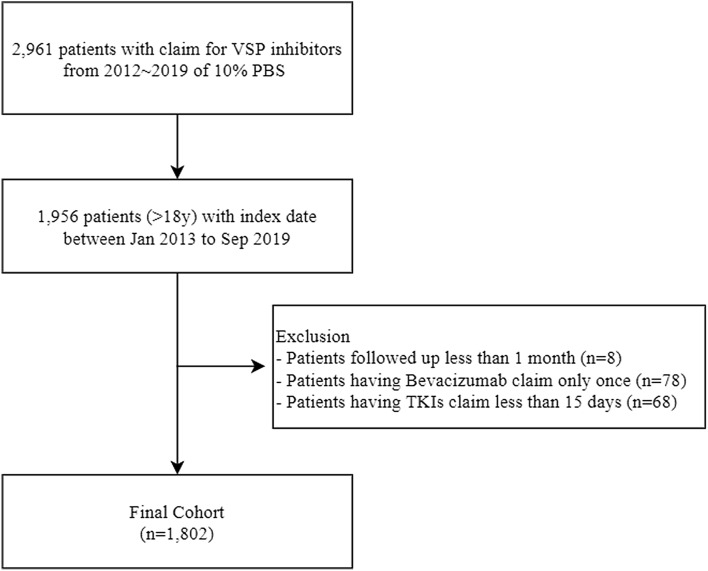
We used dispensing records for a 10% random sample of Australians to identify treatment with subsidised VSPi from 2013 to 2018. We further identified dispensings of oral antihypertensive medicines 6 months before and 12 months after VSPi therapy. We defined (i) new-onset hypertension in people first dispensed antihypertensives after VSPi and (ii) aggravated hypertension in people with prior antihypertensive use dispensed an additional, or higher strength, antihypertensive after VSPi. We applied the Fine-Gray cumulative incidence function and Cox proportional hazard regression.
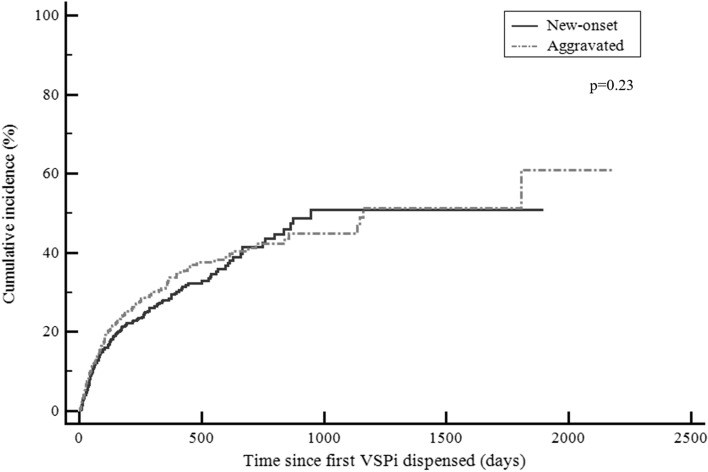
1802 patients were dispensed at least one VSPi. The mean age of the cohort was 65 years and 57% were male. The incidence of new-onset treated hypertension was 24.3% (95%CI: 21.2-27.8); age ≥ 60 years (HR 1.74; 95%CI: 1.32-2.31) and treatment with oral tyrosine kinase inhibitors compared to bevacizumab (HR 1.96; 95%CI: 1.16-3.31) were risk factors. The incidence of aggravated hypertension was 25.2% (95%CI: 22.0-28.7) and risk was elevated for patients with renal cancer (HR 2.84; 95%CI: 1.49-5.41) and cancers other than colorectal (HR 1.85; 95%CI: 1.12-3.03).
Our real-world estimates of incident hypertension appear comparable to those observed in clinical trials (21.6-23.6%). Our population-based study provides some insight into the burden of hypertension in patients commencing VSPi in routine practice.
临床试验报告称,系统性高血压是使用血管信号通路抑制剂(VSPi)的一种不良反应。来自常规临床实践的数据有限。我们旨在估计在澳大利亚全国范围内接受VSPi治疗的癌症患者中新发和加重高血压的实际发生率及风险因素。
我们使用了澳大利亚10%随机样本的配药记录,以确定2013年至2018年期间接受补贴VSPi治疗的情况。我们进一步确定了VSPi治疗前6个月和治疗后12个月的口服抗高血压药物配药情况。我们定义了(i)在首次接受VSPi治疗后首次配用抗高血压药物的患者中的新发高血压,以及(ii)在VSPi治疗后配用额外或更高剂量抗高血压药物的既往使用抗高血压药物患者中的加重高血压。我们应用了Fine-Gray累积发病率函数和Cox比例风险回归。
1802名患者至少接受了一种VSPi治疗。该队列的平均年龄为65岁,57%为男性。新发治疗性高血压的发生率为24.3%(95%置信区间:21.2 - 27.8);年龄≥60岁(风险比1.74;95%置信区间:1.32 - 2.31)以及与贝伐单抗相比使用口服酪氨酸激酶抑制剂治疗(风险比1.96;95%置信区间:1.16 - 3.31)是风险因素。加重高血压的发生率为25.2%(95%置信区间:22.0 - 28.7),肾癌患者(风险比2.84;95%置信区间:1.49 - 5.41)和结直肠癌以外的癌症患者(风险比1.85;95%置信区间:1.12 - 3.03)的风险升高。
我们对高血压发病率的实际估计似乎与临床试验中观察到的结果相当(21.6 - 23.6%)。我们基于人群的研究为常规实践中开始使用VSPi的患者的高血压负担提供了一些见解。