Medical Oncology Department, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy.
Department of Oncology, Veneto Institute of Oncology IOV - IRCCS, Padua, Italy.
Oncologist. 2022 Feb 3;27(1):e29-e36. doi: 10.1093/oncolo/oyab012.
In patients with RAS/BRAF wild-type metastatic colorectal cancer (mCRC), growing evidence supports anti-epidermal growth factor receptor (EGFR) retreatment, whereas little is known on the outcomes of anti-EGFR-based reinduction therapy during the upfront strategy.
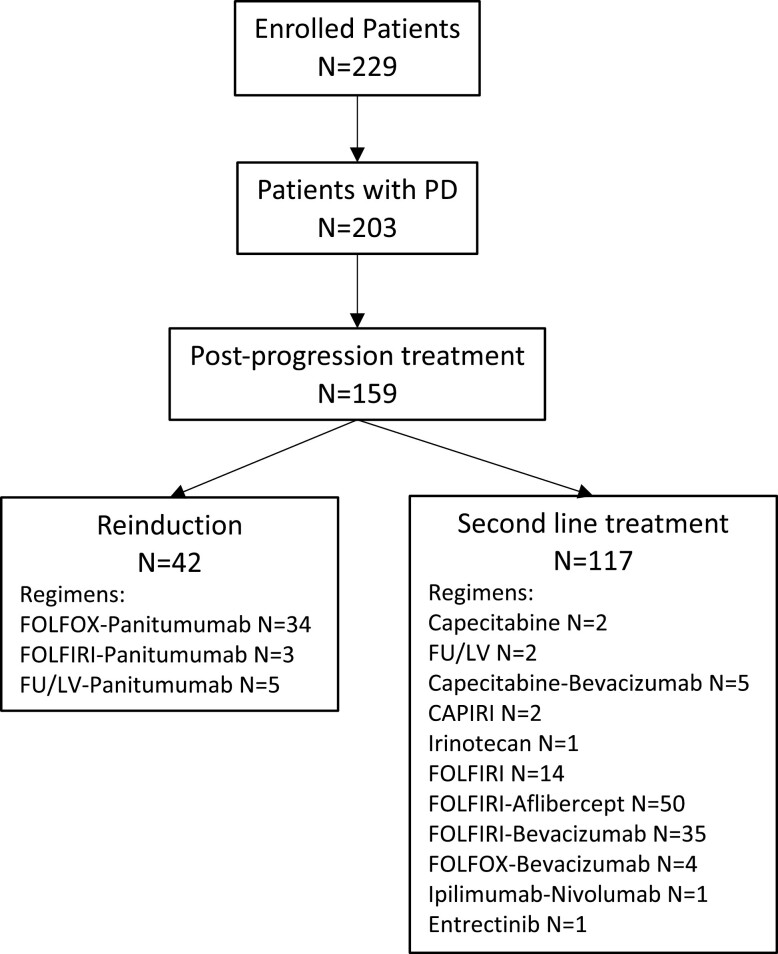
We included patients enrolled in the Valentino study who had disease progression and received at least one dose of post-progression therapy. The Kaplan-Meier method and Cox proportional hazards regression were used for the survival analysis. When comparing the outcomes of anti-EGFR-based reinduction versus any second line, a propensity score-based matching was used.
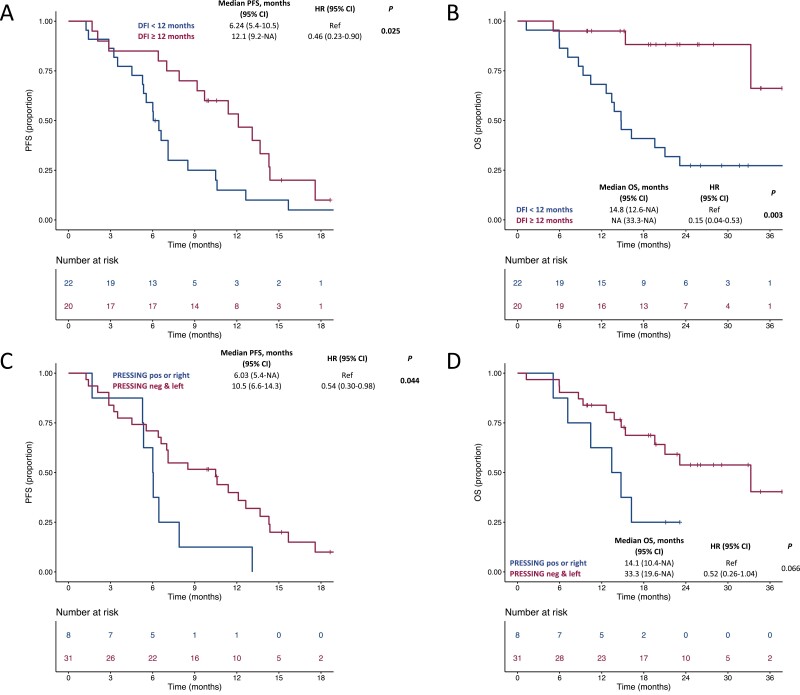
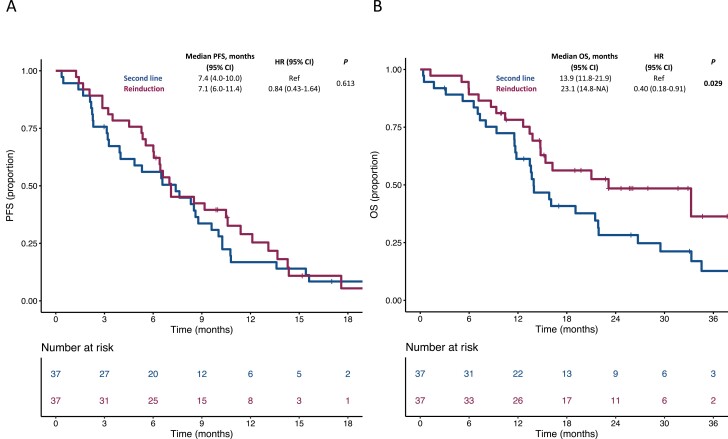
Liver-limited/single site of disease (P < .001 and P = .002), left-sidedness (P = .029), surgery of metastases (P = .003), early tumor shrinkage, and deeper responses (P = .018 and P = .036) were associated with the use of anti-EGFR-based reinduction versus any other second line. All patients treated with reinduction had an anti-EGFR-free interval of at least 3 months. In the propensity score-matched population, progression-free survival (PFS) was similar in the 2 treatment groups, the overall survival (OS) was significantly longer for patients treated with reinduction (P = .029), and the response rate was higher in patients treated with reinduction (P = .033). An oxaliplatin-free interval ≥12 months, left-sidedness, and molecular hyperselection beyond RAS/BRAF were associated with significantly better outcomes after anti-EGFR-based reinduction.
Reinduction strategies with anti-EGFR-based regimens are commonly used in clinical practice. Our data highlight the importance of clinical-molecular selection for re-treatments and the need for prospective strategy trials in selected populations.
在 RAS/BRAF 野生型转移性结直肠癌(mCRC)患者中,越来越多的证据支持抗表皮生长因子受体(EGFR)的再治疗,而对于一线策略中基于抗 EGFR 的再诱导治疗的结果知之甚少。
我们纳入了 Valentino 研究中疾病进展并接受至少一次后进展治疗的患者。采用 Kaplan-Meier 法和 Cox 比例风险回归进行生存分析。当比较基于抗 EGFR 的再诱导与任何二线治疗的结果时,使用倾向评分匹配。
肝局限性/单一疾病部位(P<0.001 和 P=0.002)、左侧(P=0.029)、转移灶手术(P=0.003)、早期肿瘤退缩和更深的反应(P=0.018 和 P=0.036)与基于抗 EGFR 的再诱导与任何其他二线治疗的使用相关。所有接受再诱导治疗的患者均有至少 3 个月的无抗 EGFR 间期。在倾向评分匹配的人群中,两组的无进展生存期(PFS)相似,再诱导治疗的患者总生存期(OS)显著更长(P=0.029),再诱导治疗的患者缓解率更高(P=0.033)。奥沙利铂无间期≥12 个月、左侧和除 RAS/BRAF 以外的分子超选择与基于抗 EGFR 的再诱导后的更好结果相关。
基于抗 EGFR 的方案的再诱导策略在临床实践中常用。我们的数据强调了为再治疗进行临床-分子选择的重要性,以及在选定人群中进行前瞻性策略试验的必要性。