Holleman Marscha S, Huygens Simone A, Al Maiwenn J, Kuppen Malou C P, Westgeest Hans M, van den Bergh Alfonsus C M, Bergman Andries M, van den Eertwegh Alfonsus J M, Hendriks Mathijs P, Lampe Menuhin I, Mehra Niven, van Moorselaar Reindert J A, van Oort Inge M, Somford Diederik M, de Wit Ronald, van de Wouw Agnes J, Gerritsen Winald R, Groot Carin A Uyl-de
Erasmus School of Health Policy and Management, Erasmus University Rotterdam, Rotterdam, The Netherlands.
Institute for Medical Technology Assessment, Erasmus University Rotterdam, Rotterdam, The Netherlands.
Drugs Real World Outcomes. 2022 Jun;9(2):275-285. doi: 10.1007/s40801-022-00294-7. Epub 2022 Mar 21.
Real-world disease models spanning multiple treatment lines can provide insight into the (cost) effectiveness of treatment sequences in clinical practice.
Our objective was to explore whether a disease model based solely on real-world data (RWD) could be used to estimate the effectiveness of treatments for patients with castration-resistant prostate cancer (CRPC) that could then be suitably used in a cost-effectiveness analysis.
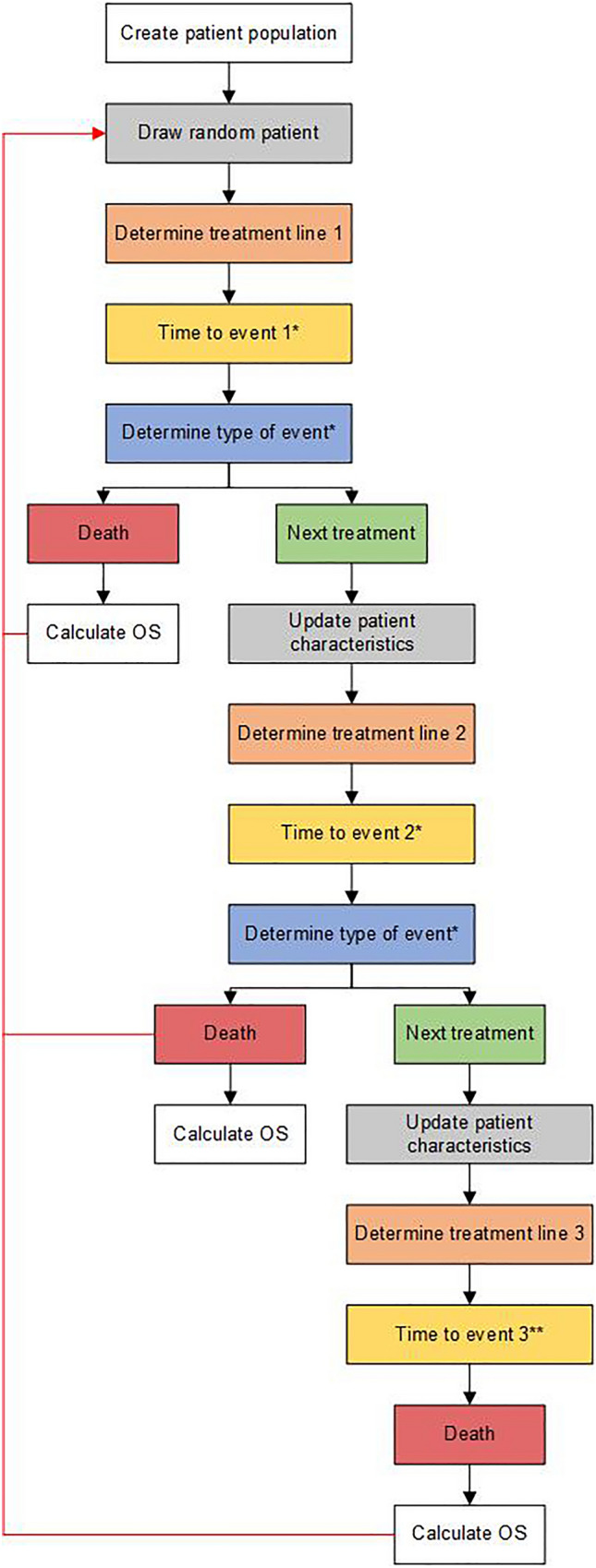
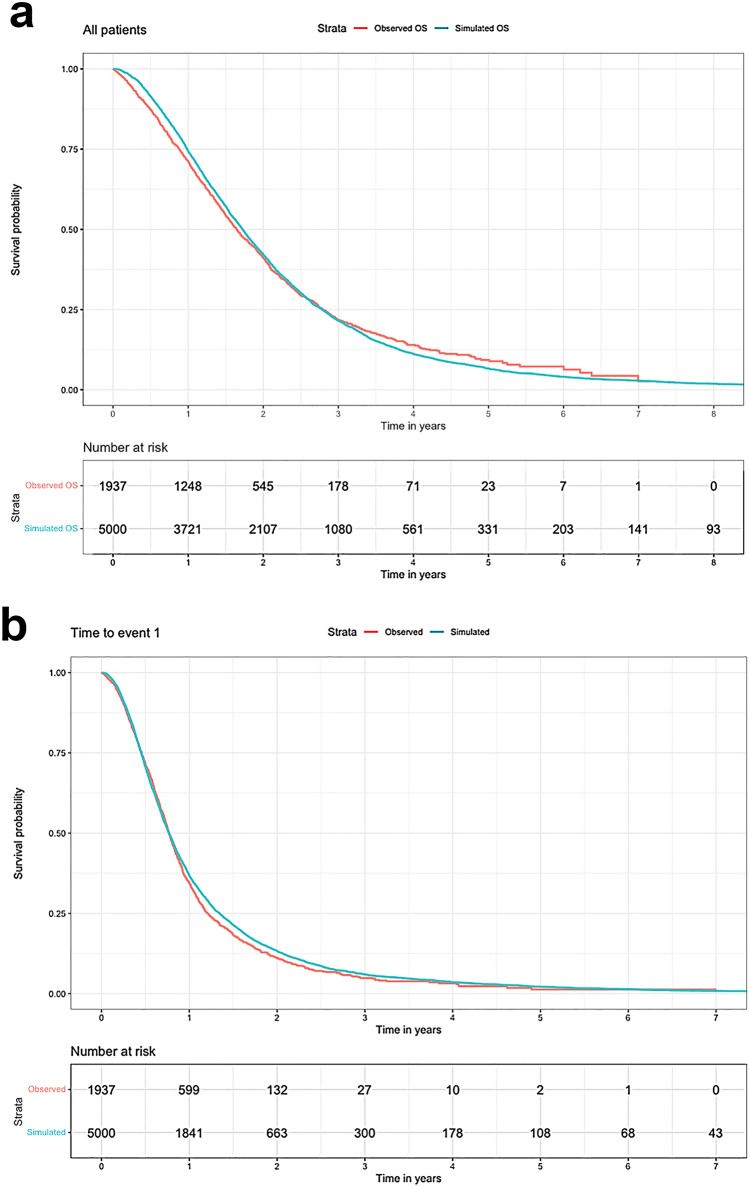
We developed a patient-level simulation model using patient-level data from the Dutch CAPRI registry as input parameters. Time to event (TTE) and overall survival (OS) were estimated with multivariate regression models, and type of event (i.e., next treatment or death) was estimated with multivariate logistic regression models. To test internal validity, TTE and OS from the simulation model were compared with the observed outcomes in the registry.
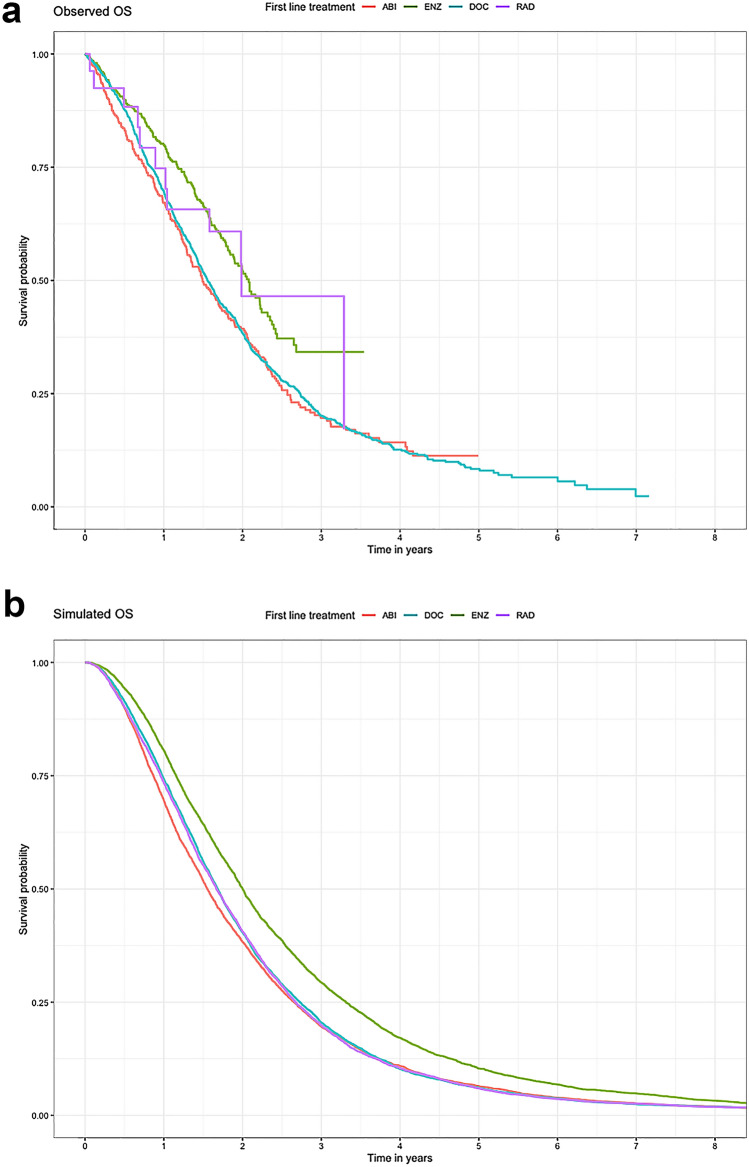
Although patient characteristics and survival outcomes of the simulated data were comparable to those in the observed data (median OS 20.6 vs. 19.8 months, respectively), the disease model was less accurate in estimating differences between treatments (median OS simulated vs. observed population: 18.6 vs. 17.9 [abiraterone acetate plus prednisone], 24.0 vs. 25.0 [enzalutamide], 20.2 vs. 18.7 [docetaxel], and 20.0 vs. 23.8 months [radium-223]).
Overall, the disease model accurately approximated the observed data in the total CRPC population. However, the disease model was unable to predict differences in survival between treatments due to unobserved differences. Therefore, the model is not suitable for cost-effectiveness analysis of CRPC treatment. Using a combination of RWD and data from randomised controlled trials to estimate treatment effectiveness may improve the model.
涵盖多个治疗线的真实世界疾病模型能够为临床实践中治疗序列的(成本)效益提供见解。
我们的目的是探究仅基于真实世界数据(RWD)的疾病模型是否可用于估计去势抵抗性前列腺癌(CRPC)患者的治疗效果,进而适用于成本效益分析。
我们使用来自荷兰CAPRI登记处的患者水平数据作为输入参数,开发了一个患者水平模拟模型。通过多变量回归模型估计事件发生时间(TTE)和总生存期(OS),并通过多变量逻辑回归模型估计事件类型(即下一次治疗或死亡)。为检验内部有效性,将模拟模型的TTE和OS与登记处观察到的结果进行比较。
尽管模拟数据的患者特征和生存结果与观察数据相当(中位OS分别为20.6个月和19.8个月),但疾病模型在估计治疗之间的差异时准确性较低(模拟人群与观察人群的中位OS:阿比特龙加泼尼松为18.6个月对17.9个月,恩杂鲁胺为24.0个月对25.0个月,多西他赛为20.2个月对18.7个月,镭-223为20.0个月对23.8个月)。
总体而言,疾病模型准确地近似了CRPC总人群中的观察数据。然而,由于未观察到的差异,疾病模型无法预测治疗之间的生存差异。因此,该模型不适用于CRPC治疗的成本效益分析。结合RWD和随机对照试验数据来估计治疗效果可能会改进该模型。